
INTRODUCTION
The opening years of the new century have proved exceptionally difficult for the tourism industry in South East Asia due to a series of crises within and outside the region which have had direct and indirect impacts. These include the 2001 terrorist attacks in the USA, the Bali bombings in 2002, the Iraq war and its aftermath and the Indian Ocean tsunami in 2004. Another serious crisis was the outbreak in 2003 of Severe Acute Respiratory Syndrome (SARS), a new and potentially deadly virus. This damaged tourism across the world, but especially in those Asian countries at the centre of the epidemic. Vietnam was one such destination and this paper examines the consequences of SARS for tourism there and the responses of the industry to the emergent challenges.
After a brief review of the literature, an introduction to tourism in Vietnam and the nature and implications of SARS is provided. Reactions of tourism enterprises to the threat it posed are then discussed in terms of health and safety, finance, human resources and marketing. The effectiveness of these efforts is reviewed and a final section presents a tentative crisis management campaign model which might be adapted for use in the future. Findings are based on personal interviews with selected industry representatives, supported by secondary material from an assortment of
Address correspondence to Joan C. Henderson, Nanyang Business School, Nanyang Technological University Nanyang Avenue, Singapore 639798. Email: ahenderson@ntu.edu.sg
published sources. While the medical battle against SARS was successful, there is a possibility of its recurrence or the emergence of another similar viral infection. The topic is therefore timely and of wider interest as all destinations must prepare for such eventualities.
RESEARCH METHODOLOGY
Primary data was obtained from five in depth interviews with senior managers from a leading international hotel in Hanoi, the national airline and one of the major entertainment parks in Ho Chi Minh City. Several other organisations were contacted, including the Vietnam Tourism Administration (VNTA), but either failed to respond or refused the request for a meeting. The semi-structured interview comprised questions about the effect of SARS on the business in 2003, the various measures adopted to deal with the crisis and the difficulties encountered. Comments were also invited about the existence of any crisis management plans and their merits. Interviews were selected as an appropriate methodology because they facilitate full exploration of the issues and allow for personal reflections and evaluation, providing observations from an insider perspective which might otherwise not have been available.
Some limitations of the study must be acknowledged such as the very small number of interviews and restrictions imposed due to confidentiality. While participants were generally very helpful in sharing details about their company's experiences of SARS, there was a reluctance to disclose certain statistics relating to finance. The passage of time may also have undermined the recall of the interviewees because discussions took place in late 2004 and early 2005, almost two years after SARS. Nevertheless, much useful material was collected which affords valuable insights into the dynamics of a Southeast Asian tourism crisis related to health and approaches to its management.
LITERATURE REVIEW
Crisis seems to have become a defining feature of the modern world in general and tourism has proved itself vulnerable to problems arising in the internal and external environments. Economic turbulence, political instability, social unrest, terrorism, health scares and extreme weather have all deterred tourists and disrupted the operation of the industry. There has been a reluctance in the past to accept and act upon this tendency to crisis (Cassedy, 1991) or downplay actual and potential hazards in order to avoid adverse publicity and commercial losses. However, such a stance is increasingly untenable and the subject of tourism crises and their management has recently been attracting much greater interest from academics and practitioners (Glaesser, 2004; Laws et al, 2007; Ritchie, 2004; Wilks et al, 2006).
There is already a substantial literature on crisis management in general (Booth, 1993; Harvard Business School, 2004) and this is now being applied to tourism, including within a South East Asian context (Nankervis, 2000). Commentators stress the importance of perceptions of safety and security regarding individual tourist behaviour and investment decisions. Destinations where there are doubts about personal safety face an erosion of confidence, a tarnished image and falling arrivals which may degenerate into crisis. Terrorism is a prime concern, but alarms over health may be equally detrimental if sufficiently grave (Clift and Page, 1996). The role of the media is frequently highlighted and the amount and tone of publicity can help to determine the intensity of a crisis and the speed of resolution (Herrero and Pratt; 1998).
Several authors propose guidelines for anticipating and managing crises (Beirman, 2003; PATA, 2003), incorporating a corporate communications strategy, and Faulkner's (2001) framework
pertaining to a natural disaster is one of the most often cited. However, many proposals appear either excessively broad or too tied to specific situations (de Sausmarez, 2003) and devising a plan that is capable of adaptation to suit a range of scenarios is an ongoing challenge for the tourism industry and individual businesses.
VIETNAM'S TOURISM INDUSTRY AND THE IMPACT OF SARS
Tourism in Vietnam has advanced considerably since the introduction of 'doi moi' or economic restructuring in 1986 when there were only 54,353 overseas visitors (Nguyen Van Binh and Le Van Minh, 1997). Numbers crossed the million mark in 1994 and had exceeded two million by 2000, rising to 2.6 million in 2002 (VNTA, 2005). The industry is of growing importance economically as a generator of income and attractor of foreign direct investment nationally and locally. Large numbers are also employed in this labour intensive sector, especially younger workers who might otherwise be unemployed. It accounted for an estimated 3.5% of Vietnam's GDP in 2000 and the World Travel and Tourism Council (WTTC, 2005) expects the overall tourism economy to have contributed at least 8% of GDP in 2004, with forecasts that the industry has the capacity to expand at an annual rate of 8.3%.
Such figures suggest the significance of the tourism industry and the reasons for concern about any downturn as a result of unexpected crisis. Vietnam's strengths as a destination include relative safety and security, alongside outstanding natural and cultural attractions. It is seen as immune from the threat of terrorist attacks associated with Islamic extremism which has tarnished rival destinations in the region. However, the reputation as a place of personal safety was called into question by SARS which evolved from a public health crisis into a tourism crisis of international dimensions.
SARS is a contagious viral respiratory illness which is now known to be a consequence of the corona virus and believed to be spread by vapour droplets, usually amongst people in close personal contact. It can be fatal, but the mortality rate is not as high as originally thought and 774 have died out of a total of 8,098 people worldwide contracting the disease (CDC, 2004). The illness seems to have originated in the southern Chinese province of Guangdong at the end of 2002 and was carried to Vietnam by a returning businessman who had stayed at the same Guandong hotel as an infected local physician. The victim was hospitalised at the French Hospital in Hanoi and initially diagnosed as having atypical pneumonia on 26 February, but this was subsequently confirmed to be SARS. Some of the staff who attended the patient caught the virus and there were 40 cases and five deaths at the hospital (WHO, 2003a).
The disease was a mystery at the beginning, without any vaccine or cure, and the manner in which it crossed the Chinese border and established itself in Hong Kong, Singapore, Taiwan and Toronto in addition to Vietnam generated great anxiety. It appeared to be out of control, moving at speed along international air routes. The World Health Organisation (WHO) issued a global alert on 12 March and sent a multidisciplinary outbreak control team to Vietnam. The authorities there were praised for their transparency, prompt communication and cooperation with the WHO and implementation of a regime of rapid detection, immediate isolation, infection control and vigorous contact tracing (WHO, 2003a). As a result, the outbreak was contained within the hospital and Vietnam was the first country to be removed from the WHO's list of infected areas on 28 April 2003. Worries still lingered as local transmission continued in other parts of the region and there was uncertainty about the future. Predictions of a worldwide pandemic were not realised, however, and there were no further instances after July 2003 with the exception of a few isolated cases in China.
It is not surprising that SARS had an immediate effect on tourism across Asia as people were unwilling to travel, especially by air, for fear of catching the virus. The worst hit areas were shunned and outbound travellers from these zones were subject to screening and restrictions. Media publicity and formal warnings from governments and official agencies heightened perceptions of danger, sometimes out of proportion to actual risks (Pine and McKercher, 2004). This is demonstrated by Vietnam where tourism was damaged by cancellations of holiday and business trips, even though numbers afflicted by SARS were extremely small. Table 1 reveals the decline in arrivals for 2003 compared to 2002, May being the worst month when tourists and revenues fell dramatically.
Table 1 Vietnam International Tourist Arrivals by Month 2002-2003
| Month | 2002 | 2003 |
|---|---|---|
| First Quarter | 639,249 | 709,419 |
| January | 198,870 | 245,937 |
| February | 223,891 | 247,199 |
| March | 216,488 | 216,283 |
| Second Quarter | 659,355 | 364,595 |
| April | 222,299 | 158,186 |
| May | 217,169 | 99,816 |
| June | 219,887 | 106,593 |
| Third Quarter | 673,676 | 556,786 |
| July | 225,726 | 153,530 |
| August | 238,488 | 193,584 |
| September | 209,462 | 209,672 |
| Fourth Quarter | 655,708 | 797,935 |
| October | 199,471 | 225,938 |
| November | 223,062 | 276,961 |
| December | 233,175 | 295,036 |
| Total | 2,627,988 | 2,428,735 |
Source: VNTA, 2005
Arrivals were depressed until September and the year saw a contraction of 7.6%, according to official statistics, although some analysts have indicated a higher figure of 16% (AFP, 2004). Nevertheless, recovery of the industry as a whole was evident in the final months of 2003 and sustained in 2004 when 2.9 million international visitors were recorded (EIU, 2005).
RESPONSES TO SARS
The adverse developments in 2003 obviously had implications for the organisations involved in the interviews and there was very limited knowledge of SARS or how long it would persist at the onset. The surveyed hotel was unaffected in the first quarter, but average occupancy dropped from 80% to less than 20% in April and May when revenue per available room was 75% below normal. Second quarter revenues for the surveyed airline also shrank by almost half in the first three months of the year due to an absence of bookings and cancelled journeys. In the case of the surveyed park, attendance fell by an estimated 3-5%. However, return to normality was fairly rapid and trade had been restored to its usual level at the hotel by June. The surveyed airline reported a 67.5% surge in its third quarter revenues and carried about the same number of passengers in 2003 as had been anticipated prior to the discovery of SARS. The steps taken by the three businesses in reaction to SARS are outlined below and represent a foundation for later suggestions about managing crisis in the tourism industry in general.
Health and Safety
SARS was an issue of both hygiene and lack of understanding and the hotel invited the Director of Vietnam's Central Hygiene and Epidemiology Institute to give a talk to staff about the virus and how they could protect themselves. Details about prevention were communicated to all employees via notice boards. Room and kitchen staff were ordered to wear masks when working and disinfection chemicals were sprayed regularly in public areas. Foreigners were required to present their health certificates to guarantee that no infected guests came into the hotel undetected and staff were also checked for symptoms such as fever. Suspected cases were tracked by individual managers until they were cleared.
With regard to the airline, the primary aim in the early phase was to gather information about SARS to assist in coping with it. Essential details were obtained from the Ministry of Health, the VNTA and other government institutions. The press and tourism partners were also a source of feedback about popular attitudes and behaviour at home and abroad. Precedence was then given to the implementation of recommended health and safety measures regarding both employees and passengers. For example, the WHO advised that good personal hygiene should be observed by everyone, face masks worn if there was a possibility of cases on board a flight and aircraft be thoroughly cleansed and disinfected (WHO, 2003b).
The park management also sought facts about the epidemic and its progress from newspapers and television. The business development staff asked for the opinions of partner tour operators and tour guides who dealt directly with tourists. Based on the material and directives from the local authority, preventive procedures were put in place. Due to unanswered questions about the means of transmission, potential disease carrying animals were isolated and the park grounds were disinfected. The programme-content team modified what was on offer and exercised supervision over customer movements in the light of the possible new hazards.
Financial
The hotel attempted to minimise all short term expenditure and non-urgent purchases were halted. Utility costs were reduced and vacant floors were taken out of service. The budgets for domestic advertising and public relations were also trimmed. In contrast, the airline's president revealed plans to buy five aircraft in a decision which seemed to contradict a general trend of financial restraint in the civil aviation industry. The company was confident that SARS would not last long and was taking the opportunity of competitive prices to rejuvenate its fleet and prepare for a comeback. Flights, however, were cut and schedules revised as demand slumped. The park's management also recorded increased spending, principally in the areas of health and safety and marketing.
Human Resources
There were no retrenchments at the hotel which did not have part-time employees or attachments at the time. Releasing permanent staff was only considered as a last resort because of undesirable human resources repercussions. However, employees were encouraged to take their full entitlement of paid leave and managers volunteered to go on extended unpaid leave. The airline and the park
management also both agreed that the scale of the crisis did not warrant termination of contracts. A close watch was kept on staff health and anyone feeling sick was instructed to leave immediately and get proper medical treatment before returning to work.
Marketing
In order to improve occupancies, the hotel introduced a scheme whereby guests who stayed for one night at the standard charge could choose how much to pay for an additional night's accommodation from US$1 to US$99. Ten rooms were devoted to the project which lasted ten days and they were fully booked almost immediately, many by customers new to the hotel. The story attracted a great deal of media publicity, although not all was favourable with some reports describing how five star properties were now competing with single star hotels and implying a corresponding diminution in service quality. The hotel also participated in an industry-wide promotional campaign along with other leading hotels, tour operators and transport companies which enabled those paying for a three night package to enjoy another night at no extra cost.
Management realised that corporate customers were more reliable and consistent than leisure travellers during the crisis, the latter displaying a much greater propensity to cancel. The focus of marketing and sales was redirected accordingly to the corporate travel group and the proportion of business it accounted for rose from 50% to 60% . There was also a decision to diversify markets geographically and reach out to Australia, Europe and Korea instead of concentrating on Japan. The underlying rationale was that a broader base of customers would minimise the danger of over-dependence, especially on such risk averse tourists as the Japanese, should a crisis be repeated.
Initially the airline marketing department was preoccupied with an intensive promotional campaign to commence when the crisis was over. It also organised some promotions aimed at the domestic market, although these did not appear to have much of an impact. Once the outbreak was declared formally at an end by the WHO in 2003, the airline cooperated with the VNTA to convey the message that Vietnam was safe as the first 'SARS-free' country. It was advertised as a prime destination in the mass media of France and Japan, two of Vietnam's chief foreign markets, and on international television channels such as CNN, CNBC and NHK. The company then announced a US$1 million marketing campaign and substantial fare discounts for tourists from Australia, France, Japan and South Korea. It was also working with tour operators and hotels in Hanoi and Ho Chi Minh City, as previously noted, to provide attractively priced package deals for inbound tourists.
Marketing and Public Relations played a decisive part in the way the park coped with SARS which was essentially a crisis of fear in the south given that the disease did not extend beyond Hanoi. The public was constantly informed through broadcast and print media that there were no health risks and the site was safe to visit. In addition, money was spent on product development to create new and appealing attractions and special offers, such as reduced entry charges, were available. Children were the main target of promotion since they were judged to be the key decision makers regarding family holiday activities.
REVIEW
As indicated by the above account, health and safety were one of the top priorities for those interviewed. Strict guidelines were devised and followed, in accordance with official instructions, about SARS prevention and protection. Regimes of cleaning and disinfecting were installed to maintain the highest standards of hygiene. Other common measures included cost savings, although the airline took the opportunity to invest heavily in new planes. Operations were revised in line with the fall in demand, including the rationalisation of services and reduction of capacities. Marketing was shaped by the stage of the crisis, linked to the history of the SARS outbreak. There were a series of campaigns and price discounts intended to stimulate domestic and international arrivals, as well as allay the fears of tourists and the industry in generating markets.
All the organisations studied claimed to have effective crisis management strategies which they were able to employ during the SARS period. The hotel management regarded its response as satisfactory and felt that the necessary steps had been taken in a timely fashion. The general emergency guidelines supplied by the parent company had been applied to local conditions and allowed the directors to deal with SARS. It was admitted that the park did not suffer as much as its counterparts in the north and further benefited from the fact that much of its custom came from the domestic market of residents from Ho Chi Minh City and the surrounding provinces. Nevertheless, the management believed that it too had been suitably proactive and handled the actual and potential risks with competence. Appropriate procedures had been formulated and enforced and negative publicity had been kept to a minimum.
The actions and achievements of specific organisations must be assessed against the background of moves made by the industry as a whole under the leadership of the VNTA. Attempts to arrange an interview with a senior VNTA official were unsuccessful as previously noted, but it appears that the organisation cooperated with the Ministry of Health to issue and implement hygiene directives and procedures intended to assist businesses in coping with SARS. Tourism enterprises at home and abroad received regular and reliable information about the state of SARS in Vietnam and the region. They and their customers were reassured that every effort was being made to defeat the disease. Many journalists were invited to the country to see the situation for themselves, facilitating more accurate reporting. Hotels and local tour firms arranged a variety of discounts and there were a number of collaborations. Development was also stimulated by accelerated planning of those new resorts scheduled for completion in the years until 2010, attendance at international meetings and greater cooperation externally (BBC, 2003).
The government carefully monitored international movements, with particular reference to the border with China where officials were struggling to bring SARS under control. Health certificates and forms were demanded from Chinese visitors and Quang Ninh Province, the location of the renowned Ha Long Bay where the Chinese usually made up 60% of tourists, barred them (The Straits Times, 2003). Large scale festivals intended to attract mass audiences were also limited at the height of the crisis when there were doubts about whether the outbreak had been contained (Saigon Times, 2003).
While the return to health of tourism by the year end would seem to confirm the views of interviewees about success in handling the crisis, there are other factors to consider. These relate to the extent of the crisis and the political commitment to combat it, given that the crisis was one which originated outside of tourism and demanded a response from the public sector nationwide. The situation in Vietnam was not as grave as that confronting destinations with community transmission of SARS, such as Hong Kong and Singapore, and resident and tourist anxieties were thus more easily addressed. Despite the country's less developed status, the Vietnamese government was quick to react and open in its communications. Its approach helped to gain the confidence and trust of citizens and the international community (The Straits Times, 2003). Much of the recovery of tourism can therefore be attributed to the relatively short duration of the SARS outbreak and the actions of non-tourism bodies. The importance of additional influences must also be stressed, not least an economy which was expected to thrive and therefore of great interest to foreign businessmen and investors who were keen to resume visits for commercial purposes.
It has already been observed that SARS was a crisis for several other countries in East Asia and for the region as a whole as well as destinations beyond. A comprehensive review of the circumstances and handling of the crisis outside Vietnam is beyond the scope of this study, although reports indicate that governments and the tourism industry tended to follow a common approach regarding its management and especially in terms of marketing for recovery (Henderson, 2003; Pine and McKercher, 2004; WTO, 2003). Experiences recounted reveal the importance of travel advisories in the return to normality and the SARS-free announcements by the WHO were hailed as a major step forward, suggesting the influence such warnings can exert over tourism flows and the imperative of exercising caution over their imposition (PATA, 2005).
CRISIS MANAGEMENT CAMPAIGN MODEL
Taking into consideration the policies implemented during the SARS period in Vietnam, a recommended mechanism and set of measures for dealing with crisis have been identified. These have a wider applicability and could be adopted at a unit, corporate or industry level. Crisis management can be conceived of as a special campaign in which human, financial, operational and other resources are drawn on in order to deal with the difficulties. The ultimate aim is to overcome the threats imposed by the crisis and take advantage of any opportunities; as well as a time for solving immediate problems, crisis may be a chance for positive change and growth. An original model is depicted in Figure 1 and comprises four activity centres, the proposed functions of which are summarised in this section. Although the contribution of each centre will vary depending on the phase of the crisis, all must work simultaneously and cooperate under the direction of strong leadership. The model is derived from the research findings and is based upon the various accounts of crisis management in theory and practice made reference to in the literature review.
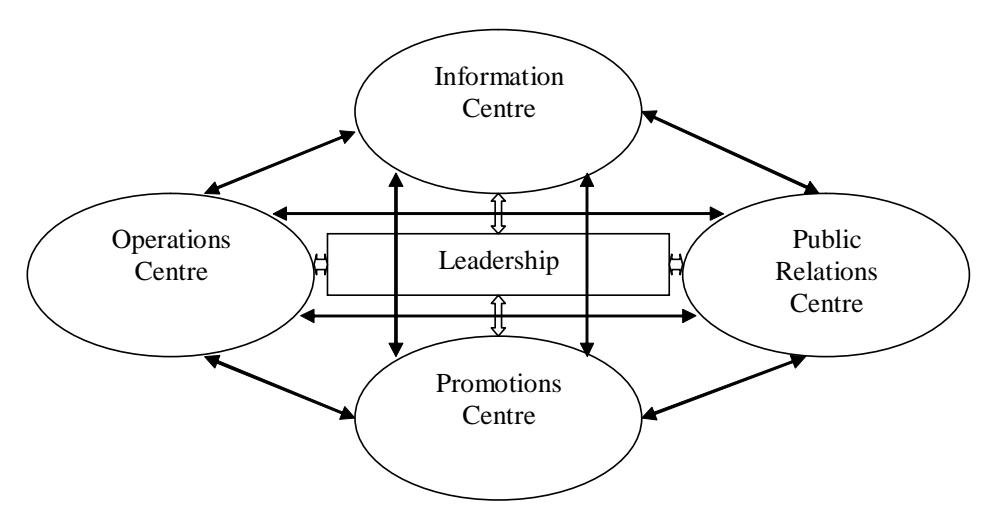
Figure 1 Crisis Management Campaign Model
Information Centre (IC)
A Crisis Management Campaign (CMC) starts when news of a possible crisis reaches the company's IC. Any employee of the company is a part of this centre, providing it with relevant information obtained from various channels. The material should be analysed and synthesised in a summary to be distributed to the other centres and the CMC leader. The leadership then will have to decide if conditions call for the launching of a CMC and, if so, the IC has to collect useful data about the cause and nature of the crisis and the issues to be addressed. The material acts as the foundation of a plan, devised after consultation with all the centre heads, which will attempt to answer questions such as how the crisis will affect the company, its duration, the seriousness of the threats and ways of meeting these. As the situation evolves and new information emerges, the CMC plan must be adjusted. The vital role of intelligence is demonstrated by SARS, about which there was initial ignorance. Rapid advances in knowledge were made by scientists around the globe as the epidemic ran its course which the tourism industry needed to be aware of if it was to combat the disease and fears of it.
Operations Centre (OC)
When the plan has been finalised, the next task is to act immediately to try to avert the crisis or constrain the damage if prevention is not a realistic option. These endeavours should be the responsibility of an OC which takes care of the practicalities of the crisis such as safeguarding lives, property and equipment. Compensation matters also have to be decided upon to placate customers and discourage them from engaging in litigation, hence hurting the corporate image. Everyone should be fully informed and updated about OC moves and there must be a constant exchange of information amongst the centres overall.
The OC has the additional task of ensuring that operations are conducted with the objective of optimal use of resources and the realisation of any financial gains. While there is a tendency for companies in crisis to cut back operations to avoid incurring unnecessary costs and minimise expenditure, there may be scope for revenue generation and spending with a view to longer term returns. Staff could be sent for retraining, premises could be refurbished and purchases could be made, taking advantage of lower prices arising from difficult market conditions. The domestic market, sometimes neglected due to an emphasis on international tourism, could also be exploited. A good CMC should thus seek to capitalise on commercial opportunities which can be present even in the most serious of crises.
Public Relations Centre (PRC)
At the same time as gathering information and running operations, companies should cultivate good relations with the media and public. Failure to manage external communications may mar a company's reputation and even jeopardise its existence. Perceptions of a lack of transparency can lead to suspicions that a company has something to hide, thereby creating distrust. Failure to convincingly convey what the company is doing right is another harmful error and it is the job of the PRC to stop such mistakes from occurring. One person in the centre should be appointed as spokesperson for the whole CMC, working closely with the leader. This person should be responsible for dealing with the media and public, making sure that the company is as open and honest as circumstances permit. They can also be a feedback channel, passing comments back to the OC so that concerns are dealt with promptly.
Promotions Centre (PC)
The PC is charged with examining the reasons for changes in demand precipitated by the crisis, drawing up suitable promotions and preparing programmes to be launched when appropriate. Promotions to induce customers back once the peak of the crisis is over, to be initiated by the CMC leader, should be assembled. Timing is a crucial aspect and if the crisis is health-related, promotions are likely to be effective only when the threat has receded. Price discounting also will not persuade most travellers to put aside worries about contracting a deadly disease, but can be a powerful inducement when conditions have improved. The turning point in the SARS crisis was the WHO announcement about freedom from infection which was used as a sign by Vietnam and other destinations to intensify their marketing.
Strong Leadership
The CMC leader(s) are at the heart of the model and management process and must make important decisions about the campaign, consulting with the centre heads and coordinating their work. The leader could be the Chief Executive Officer, the Managing Director, or any senior manager; alternatively, a small group of top managers could form an executive committee. Regardless of its composition, the vital requirement is that the leadership must have power and the ability to command. It can be argued that during a crisis when timely and authoritative action is crucial, an autocratic style may be more acceptable than in normal circumstances.
CONCLUSION
Tourism is a significant industry in nearly every ASEAN country and in a world of growing uncertainties, crisis management emerges as a core management responsibility. The SARS epidemic illustrates the unpredictability of events in the outside environment to which the tourism industry is exposed, but also highlights the benefits of being alert and prepared. It is hoped that the findings and model presented here contain some helpful lessons about dealing with crises. They may also be a basis for further research designed to enhance understanding of crisis dynamics and provide practical tools for effective responses.
Strong warnings of future threats from existing and emergent epidemic prone and bacterial diseases cannot be ignored and add urgency to the subject. Avian influenza, commonly known as bird flu, is a current pressing concern. An especially virulent strain was discovered in several East and Southeast Asian countries in late 2003, leading to a number of human infections and several deaths. Although most cases in Cambodia, Hong Kong, Thailand and Vietnam have been the outcome of exposure to sick poultry, there are forecasts that it is only a matter of time before the potentially lethal virus mutates into a form which will allow human to human transmission amongst populations that have no immunity (WHO, 2005). The need for vigilance and preparedness is thus essential and planning for crisis deserves to be allocated a high priority.