
Introduction
The city of Bima, Indonesia has 33 slum-prone areas, covering an area of 26.2 hectares, which are inhabited by more than 25,000 people. The Rasanae Barat, Asakota, and Mpunda sub-districts [1], which are riverbank areas, have high slum levels. This is shown by inequality in health and welfare indicators, with the main factors being poverty, lack of access to a decent life, and weak governance [2].
In 2007, the coverage without access to sanitation in Bima City was 24.5%, which can easily be found in dense urban slums [1] and can cause environmental damage to water bodies [3] due to the disposal of domestic wastewater to rivers [4]. In urban slums, domestic wastewater is not the first priority for intervention by the government [5], while the absence of sanitation infrastructure such as latrines is not the main factor in continuing the habit of open defecation [6]. Poor quality and inappropriate design of latrines under government sanitation schemes may be an important factor but not the only reason [6]. There is also cultural diversity, while the national program ignores the cultural and social context of Indonesian society [7].
Culture is not an isolated phenomenon but interacts with other aspects such as physical space [8]. This is also the case in the Bima City slum settlements on the riverbanks. This insight may influence the acceptance of technology in society and ensure the sustainability of sanitation infrastructure [7]. Sanitation studies and programs that focus on understanding behavior and norms in communities before implementing program interventions and monitoring are important to do [9]. Better and locally relevant sanitation programs will help
Copyright ©2024 Published by IRCS - ITB ISSN: 2337-5779
J. Eng. Technol. Sci. Vol. 56, No. 2, 2024, 304-316 DOI: 10.5614/j.eng.technol.sci.2024.56.2.10
<sup>2</sup>Faculty of Environmental Engineering, Institut Teknologi Sumatera, Jalan Terusan Ryacudu, Way Huwi, Jati Agung, Lampung Selatan 35365, Indonesia
reduce existing gaps to achieve Sustainable Development Goal (SDG) number six, namely ensuring availability and sustainable management of clean water and sanitation for all.
The research in this paper was part of a study on socio-cultural analysis and community participation in riverbank slum areas on sustainable sanitation development (case study: Bima City, Nusa Tenggara Barat). This paper emphasizes the individual aspects of sanitation, especially related to domestic wastewater.
Methodology
To summarize the complexity of sanitation issues, this study used the Ottawa Charter for Sanitation Services (OCSS) framework, which is hereinafter referred to as Integrated Framework for Sanitation Services (IFSS) [10]. This research focused on individual aspects as part of socio-cultural analysis. The independent variables used to determine individual aspects of sanitation include: education [11]; income and financial condition [12]; perception [12, 13]; previous experience with the use of a latrine [15]; ability [13, 14, 16]; and feelings [16].
Research Study Areas
For this research, three urban slums along the riverbank were selected in Bima City (Figure 1). Bima City is one of two administrative cities located in Nusa Tenggara Barat Province and is located in the eastern part of Sumbawa Island with a geographical position between 8°30'-8°20'S and 118°41'-118°48'E. Bima City has five sub-districts, namely Rasanae Barat, Mpunda, Raba, Rasanae Timur, and Asakota. The city of Bima is traversed by seven rivers, three of which are major rivers with flooding risk, namely the Padolo River, the Romo River, and the Jatiwangi/Malay River.
Map of the research study area.
Neighborhood 2, 3, and 4, Sarae (Location 1)
Based on the classification, Neighborhoods 2 and 4 are areas with high density (> 200 people/ha), while Neighborhood 3 is an area with medium density (151-200 people/ha), but in the mayor's decree concerning slums states, Neighborhoods 2 and 3 are no longer designated as slums, while Neighborhood 4 is designated as a moderate slum. Nevertheless, in an assessment in the field of drinking water and domestic wastewater, the three locations showed low achievement indicators (<80% availability of safe access to drinking water and lack of wastewater management systems) [17].
Neighborhood 9 and 12, Paruga (Location 2 and 3)
Based on its classification, Neighborhood 9 is an area with a high density of >200 people/ha, while Neighborhood 12 is an area with a medium density of 151-200 people/ha. Neighborhoods 9 and 12 are medium level slum areas. Both are priority areas that will be handled in 2022 with a focus on five main infrastructure issues (roads, drainage, clean water, sanitation, and solid waste management) [18].
Methods
Figure 2 shows the research design and the methods used. The pragmatism paradigm [19] is used by involving social aspects through collaboration and practical knowledge resulting from social experiments to be applied to long-term socio-technical problems [20]. A mixed method was applied in the explanatory study, where qualitative data was used to explain and interpret quantitative results [21]. The quantitative part was carried out by a household questionnaire survey and the qualitative part was carried out by in-depth interviews (IDI) to provide an in-depth perspective on individual attitudes [22]. Health procedures were implemented considering the Covid-19 pandemic, which was still ongoing in Indonesia while the research was being conducted.
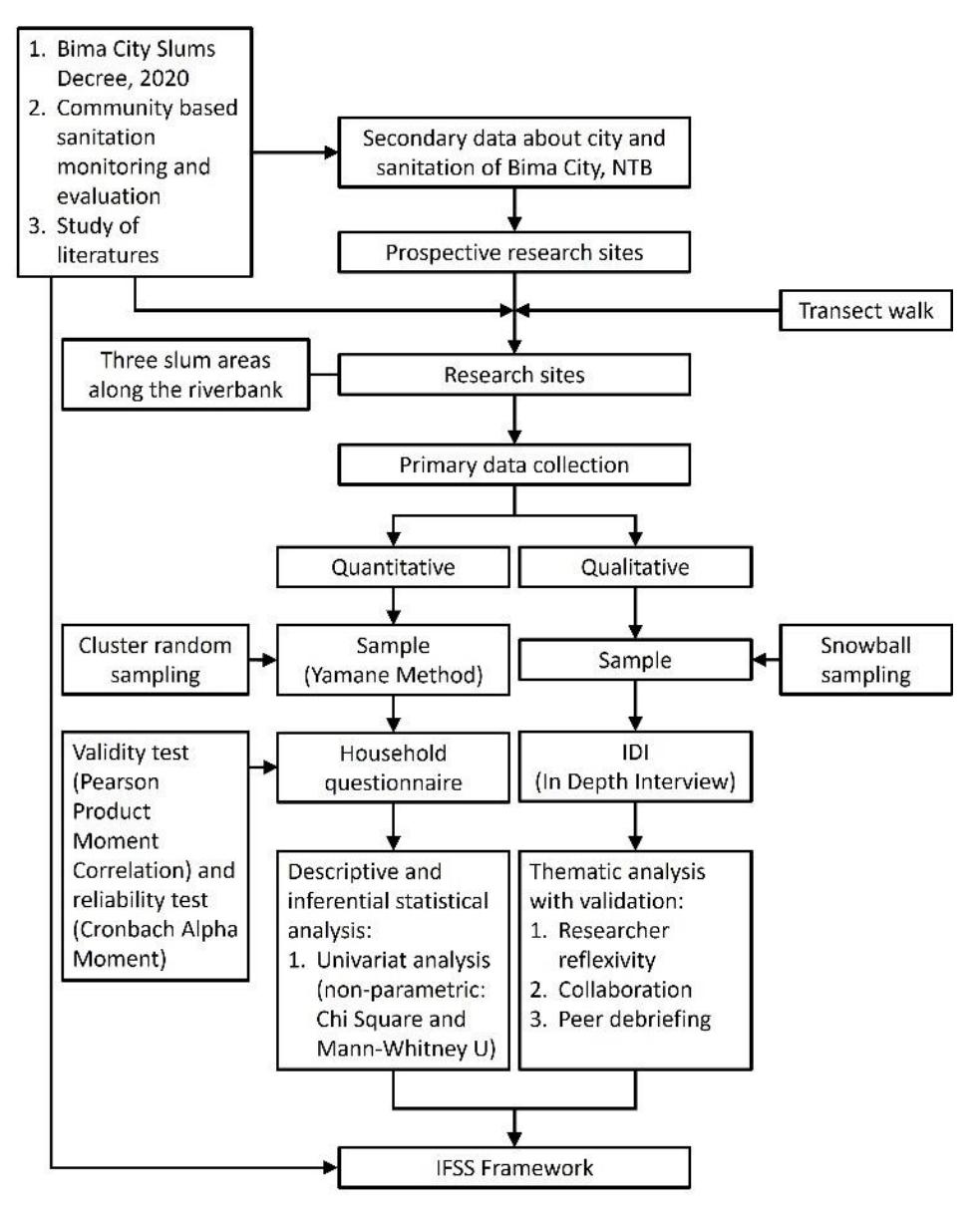
Research approach and research method.
Analysis of quantitative data was carried out using descriptive statistical analysis and inferential statistics, while analysis of qualitative data was carried out using thematic analysis. All data were then analyzed by applying the IFFS framework. The research location consisted of three riverbank slum areas with their respective characteristics, which were previously validated through a transect walk [23].
Quantitative Method
The sampling method for this research used cluster random sampling. Referring to Eq. (1), the Yamane method was used to determine the number of samples with a 95% confidence level and a population proportion of 0.5 [24]. Using this method, the estimation error was 10%, the required sample was 80 samples from a population of 385 families (Table 1) [17, 18].
\[n = \frac{N}{1 + N(e)^2} \tag{1}\]
Table 1 Population and samples.
| Locations | Household Population | Samples |
|---|---|---|
| Neighborhoods 2-4, Sarae | 229 | 48 |
| Neighborhood 9, Paruga | 98 | 20 |
| Neighborhood 12, Paruga | 58 | 12 |
| Total | 385 | 80 |
Validity and reliability were measured as evaluations [25-27]. A questionnaire pre-test was conducted on 30 respondents to detect misunderstandings, ambiguities, or other difficulties that respondents might face with the instrument [28]. Validity testing was carried out using Pearson Product Moment Correlation and reliability testing was carried out using Cronbach's alpha showing valid results (ryx ≥ 0.36, significant level 5%) and reliable (αc ≥ 0.70) [25].
Qualitative Method
Qualitative data collection was carried out through IDI using the snowball sampling method [29]. The number of samples required is shown in Table 2. This number represents the number of temporary samples, which depends on the condition of the availability of informants in the field and saturation data. Interviews were conducted with the head of the household (male) or wife (female). The interviews were recorded and then analyzed thematically by an NVivo device.
Table 2 In depth interview samples.
| Target | Neighborhood 2-4, Sarae | Neighborhood 9, Paruga | Neighborhood 12, Paruga | Total | |||
|---|---|---|---|---|---|---|---|
| M | F | M | F | M | F | ||
| Owners and users of private latrines | 2 | 2 | 2 | 2 | 2 | 2 | 12 |
| Neighbors or public latrines users | 2 | 2 | 2 | 2 | 2 | 2 | 12 |
| Open defecation | 2 | 2 | 2 | 2 | 2 | 2 | 12 |
| Key person | 2 | 0 | 2 | 0 | 2 | 0 | 6 |
| Total | 42 | ||||||
Result and Discussion
Characteristics of Respondents in Riverbank Slums in Bima City
Most household questionnaire respondents were women (85%), worked as traders (45%) and had an income of ≤IDR 750,000 per month (48%). Around 82% of respondents had a wage below the city minimum wage in 2021 (IDR 2,225,000). Occupancy in dense and slum areas in Bima City is not dominated by rented or contracted houses but own houses (79%) of the permanent type (80%) as the most common type, however, semipermanent houses (15%) are still found in the form of stilt houses. Table 3 shows the characteristics of the household questionnaire respondents.
Table 3 Characteristics of the household questionnaire respondents.
| Characteristics | n | % |
|---|---|---|
| Sex | ||
| Male | 12 | 15% |
| Female | 68 | 85% |
| Ethnic | ||
| Mbojo/Bima | 77 | 96% |
| Sumba | 2 | 3% |
| Jawa | 1 | 1% |
| Religion | ||
| Islam | 79 | 99% |
| Catholic | 1 | 1% |
| Age | ||
| 17-25 years old | 8 | 10% |
| 26-35 years old | 12 | 15% |
| 36-45 years old | 28 | 35% |
| 46-65 years old | 32 | 40% |
| Education | ||
| Non formal education | 5 | 6% |
| Elementary school | 13 | 16% |
| Junior High School | 18 | 23% |
| Senior High School/ | ||
| Vocational High School | 33 | 41% |
| University/Academy | 11 | 14% |
| Occupation | ||
| Unemployed | 20 | 25% |
| Farmer | 6 | 8% |
| Labor | 4 | 5% |
| Civil servant | 5 | 6% |
| Trader | 36 | 45% |
| Others | 9 | 11% |
| Income | ||
| ≤ IDR 750,000/month | 38 | 48% |
| IDR 750,001-1,500,000/month | 12 | 15% |
| IDR 1,500,001-2,250,000/month | 15 | 19% |
| IDR 2,250,001-3,000,000/month | 7 | 9% |
| > IDR 3,000,000/month | 8 | 10% |
| House ownership | ||
| Own | 63 | 79% |
| Family | 14 | 18% |
| Rent | 1 | 1% |
| Others | 2 | 3% |
| House type | ||
| Permanent | 64 | 80% |
| Semi-permanent | 15 | 19% |
| Others | 1 | 1% |
Clean Water and Sanitation Conditions for Riverbank Slum Communities
Communities use one to three water sources for their daily needs. Most of the drinking need is met by refill gallon water (80%); shallow wells for cooking (49%); and shallow wells for washing dishes and brushing teeth (80%). Shallow wells are used with a depth of 5-10 m (85%) and drought is experienced during the dry season of less than two weeks (42%). Economically disadvantaged people use dug wells. The community relies on groundwater because the centralized system is not running optimally, with the water not flowing at all in some research locations.
Within one family, one to four practices of defecation were found. Most respondents used a private latrine (86%) and a shared latrine (23%). The practice of open defecation (6%) was found in the three research locations, with the highest percentage directly adjacent to the river. Figure 3 shows the types of toilets in the research locations.
Most of them use septic tanks (9%), pits (64%), or dispose directly into the river (17%), which is usually done by families who live on the riverbank.
Types of closets in the research locations (left to right: seated closet, squat closet, and hole).
Individual Aspects of Riverbank Slums Communities on Sanitation Development
Based on the IFSS framework, individual aspects were broken down into five stages of sanitation, i.e., acceptability, construction, usage, maintenance, and safe disposal [15]. As for the things from all these stages that can affect sanitation development, especially the construction of latrines, among the individual aspects are perception, experience, financial ability, feelings, as well as knowledge about safe disposal.
Perceptions of Latrines and Open Defecation
Table 4 shows the respondents' perceptions of open defecation. If we consider the significance of latrine ownership, latrines owners tend to have a more negative perception of open defecation than respondents who do not have latrines. Respondents who do not have latrines tend to have the perception of being unsure or neutral towards open defecation. The significance is evident in several perceptions, such as cleanliness, private (invisible to people), not polluting, healthier, comfortable, and not spreading disease.
Table 5 shows the respondents' perceptions of latrines. If significance is calculated for latrine ownership, latrine owners tend to have a more positive perception than respondents who do not have a latrine. Significance is evident from perceptions such as the convenience of using an ordinary latrine, although both latrine owners and non-owners feel that it is comfortable.
| Latrine Ownership Total | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| No | Yes | p-value | |||||||
| n | 𝒙̅ | n | 𝒙̅ | n | 𝒙̅ | ||||
| n | 80 | 11 | 69 | ||||||
| Perception | |||||||||
| Clean | 1.41 | 1.67 | 1.17 | 0.0172 | ** | ||||
| No odor | 1.44 | 1.50 | 1.21 | 0.1152 | |||||
| Easy | 1.58 | 2.00 | 1.33 | 0.1097 | |||||
| Closed | 1.30 | 2.00 | 1.10 | 0.0009 | *** | ||||
| Acceptance | 1.56 | 1.83 | 1.24 | 0.0568 | * | ||||
| Safe | 1.38 | 2.00 | 1.10 | 0.0540 | * | ||||
| Not polluting | 1.50 | 1.83 | 1.14 | 0.0230 | ** | ||||
| Healthier | 1.50 | 1.83 | 1.19 | 0.0237 | ** | ||||
| Comfort | 1.49 | 1.83 | 1.24 | 0.0184 | ** | ||||
| Not spreading disease | 1.54 | 1.83 | 1.21 | 0.0421 | ** | ||||
Table 4 Perceptions of open defecation.
Note: *p-value <0.1 **p-value <0.05 ***p-value <0.005 (Mann-Whitney U Test)
Table 5 Perceptions of latrines.
| Latrine Ownership Total | ||||||||
|---|---|---|---|---|---|---|---|---|
| No | Yes | p-value | ||||||
| n | 𝒙̅ | n | 𝒙̅ | n | 𝒙̅ | |||
| n | 80 | 11 | 69 | |||||
| Perception | ||||||||
| Clean | 2.53 | 2.00 | 2.55 | 0.1893 | ||||
| No odor | 2.56 | 2.50 | 2.67 | 0.8710 | ||||
| Easy | 2.81 | 2.50 | 2.88 | 0.2612 | ||||
| Closed | 2.74 | 2.67 | 2.83 | 0.8207 | ||||
| Acceptance | 2.70 | 2.50 | 2.79 | 0.2101 | ||||
| Safe | 2.78 | 2.67 | 2.88 | 0.6296 | ||||
| Not polluting | 2.53 | 2.50 | 2.67 | 0.9680 | ||||
| Healthier | 2.63 | 2.50 | 2.76 | 0.5306 | ||||
| Comfort | 2.79 | 2.33 | 2.93 | 0.0019 | *** | |||
| Not spreading disease | 2.53 | 2.33 | 2.71 | 0.5954 | ||||
Note: *p-value <0.1 **p-value <0.05 ***p-value <0.005 (Mann-Whitney U Test)
The convenience factor is the only factor that intersects with perceptions about open defecation and latrines, which then influence having a latrine. Several studies have stated that the convenience factor is often successful in rural communities as well as in urban slums in encouraging the switch from open defecation to using latrines [30 31]. In the strategy to increase sanitation access through a community-based program, convenience is one of the factors that can influence changes in a person's behavior [30], so this strategy may be effective when carried out in urban slum conditions.
Previous Experience of Using a Latrine
An analysis of experience using a latrine is shown in Table 6. In terms of the intensity of using a latrine since the first experience, on a scale of 1 to 5, the average frequency was 3.74. The frequency was higher for respondents who owned latrines. Latrine owners had more intense experience using a latrine since the first experience. From the table, 9% of respondents went through a process in getting used to a latrine. Based on the IDI, they were used to defecating on the riverbank or in hanging latrines. Several reasons finally pushed them to build the latrine, as explained in the section on perceptions below.
Table 6 Previous experience using a latrine.
| Latrine Ownership | ||||||||
|---|---|---|---|---|---|---|---|---|
| Total | No | Yes | p-value | |||||
| n | % | n | % | n | % | |||
| n | 80 | 11 | 69 | |||||
| Age of using the latrine for the first time <20 years | ||||||||
| ꭓ 2 = 1.2230 | 0.2688 | |||||||
| df = 1 | ||||||||
| Yes | 73 | 91% | 11 | 14% | 62 | |||
| No | 7 | 9% | 0 | 0% | 7 | |||
| Frequency of using the latrine since the first experience | 3.74 | 2.91 | 3.87 | 0.0014 *** | ||||
Note: *p-value <0.1 **p-value <0.05 ***p-value <0.005 (Pearson's chi-squared and Mann-Whitney U Test)
The latrine usage is often started from shared latrines before finally using private latrines, such as public latrines in public facilities, communal latrines built by the government, or neighbor/family latrines. Using a shared latrine will increase the experience of using a latrine and provide benefits [13], thus encouraging to have a private latrine, although other studies that specifically discuss about communal latrines have shown the opposite, where there is a setback in implementing sanitation steps [32] due to the lack of good maintenance of communal latrines.
Finance, Perception, and Capability in Construction
As previously known, as many as 14% of respondents did not have a latrine. The main reason is that it takes a long time, or it is difficult to have enough money to build a regular and durable latrine, as shown in Table 7. The second reason, given by 82% of non-latrine owners, is that their places for defecating are now safe and private, where respondents who do not have a latrine tend to use their neighbors' latrine, as mentioned in the third reason that 73% can use the latrine of another. The fourth reason is latrine construction is difficult (64%) and most people who have latrines need a mason to build a latrine. The fifth reason is that the respondent had never thought about planning to build a latrine. These reasons are shown from rank 1 to 5 with a p-value <0.05. Table 8 shows the obstacles that affect the construction of latrines.
Table 7 Reasons for not having a latrine for non-owners of a latrine.
| Reasons for not having a latrine | n | % | Rank |
|---|---|---|---|
| 11 | |||
| It takes a long time/is difficult to have enough money to be able to build a regular and durable latrine | 11 | 100% | 1 |
| The current place for defecating is safe and closed | 9 | 82% | 2 |
| There are already other latrines that can be used | 8 | 73% | 3 |
| Building a latrine is difficult work | 7 | 64% | 4 |
| Do not know how much it costs to build a latrine | 7 | 64% | 4 |
| Many basic needs are more important | 7 | 64% | 4 |
| Never thought about building a latrine before | 6 | 55% | 5 |
| Do not really need a latrine in this area | 4 | 36% | 6 |
| Very often outside the house | 3 | 27% | 7 |
| A lot of expenses for traditional ceremonies | 2 | 18% | 8 |
| Do not have enough water to flush a latrine | 2 | 18% | 8 |
Table 8 Obstacles affecting latrine construction.
| Latrine Ownership | ||||||||
|---|---|---|---|---|---|---|---|---|
| Total | No | Yes | p-value | |||||
| n | % | n | % | n | % | |||
| n | 80 | 11 | 69 | |||||
| Cannot build their own latrine | 44 | 55% | 8 | 73% | 36 | 52% | 0.1794 | |
| Hard soil | 15 | 19% | 3 | 27% | 12 | 17% | 0.4445 | |
| It is hard to get a mason | 11 | 14% | 3 | 27% | 8 | 12% | 0.1670 | |
| Narrow land | 27 | 34% | 8 | 73% | 19 | 28% | 0.0024 | *** |
| It is difficult to bring in the materials | 20 | 25% | 8 | 73% | 12 | 17% | 0.0000 | *** |
| It is difficult to determine the location of the latrine (pamali or local belief) | 3 | 4% | 1 | 9% | 2 | 3% | 0.3288 | |
| There needs to be a traditional ceremony | 12 | 15% | 4 | 36% | 8 | 12% | 0.0204 | ** |
| Do not dare to borrow money at the bank, afraid cannot pay it back | 16 | 20% | 2 | 18% | 14 | 20% | 0.8798 | |
| Others | 35 | 44% | 10 | 91% | 25 | 36% | 0.0005 | *** |
Note: *p-value <0.1 **p-value <0.05 ***p-value <0.005 (Mann-Whitney U Test).
Based on the analysis of the significance shown in Table 7 and Table 8, several factors can be summarized that influence the construction of latrines in the three research locations from an individual perspective. These factors consist of the financial aspect [33], the perception of the place where defecation is currently used, and the ability regarding construction.
1. Financial aspects
The financial aspect is a concern for the people in the research locations considering that most of their monthly income is less than the city's minimum wage. In addition, they share their living space with family members, where 49% of them even have 5-8 family members per house. Conditions like this make them choose not to have a latrine, build one gradually, or wait for subsidies from the government. The survey results show that 76% of respondents built latrines at a cost of IDR 1-5 million. Most funding came from salaries. Respondents also borrowed money from relatives/family and bank credit (7%) and received other sources of funds, which could be in the form of government subsidies (direct cash or building materials), expenses from family, and social gathering or arisan (17%).
"…our latrine was built by the government. We are only poor people." (Woman, 72-year-old, latrine owner)
The financial aspect is an obstacle in sanitation development in urban slums [33]. A characteristic of urban slum settlements is that they have narrow alleys, so it requires more effort to deliver materials. This makes material prices higher compared to people who do not live in slum areas. The increase in material prices puts a financial burden on the community to build latrines. In this context, using local materials that are easily available is one strategy to reduce costs, for example using PET plastic bottles as a filter media for communal wastewater treatment [34-36].
2. Perceptions of the place where defecation is currently used
Based on Table 7, the second reason for not having a latrine, given by 82% of non-latrine owners, is that the current place for defecation is safe and private. Respondents who do not have a latrine tend to use their neighbors' latrine, as mentioned in the third reason and Table 8, which mention limited space, which is typical for urban slums[33]. This can trigger other reasons,such as never having thought about building a latrine before, which could have implications for other factors beyond the perception aspect [31]. Compared to open defecation, using other people's latrines, who generally have a family relation, feels safer, and more private.
"A latrine is more comfortable. Without a latrine, maybe when you were a kid you didn't feel ashamed, right? When we are adults, we do feel ashamed, especially when people pass by. […] especially as women we should be covered when we use a latrine. It's safe especially for us. Safe and comfortable." (Woman, 26-year-old, shared latrine user)
3. Construction capability
64% of household questionnaire respondents who did not have a latrine said that building a latrine is a difficult job. As much as 81% of the latrine construction process in the research locations was done by masons. The workers involved in the construction of the latrines had varied relationships, which could be family or neighbors. To reduce construction costs in view of financial limitations, the community usually builds latrines in cooperation with surrounding families. This is in line with the character of the Bima people, who usually live close to family. Their living patterns, which are still found in several areas in Bima City, involve living in housing complexes occupied by large groups of people who have close family relationships [37].
In sanitation development, culture and tradition (adat) strongly influence sanitation behavior [7, 8], especially in rural areas [15]. This is also still felt by the Bima community in urban slums. Culture is shown in the cooperation attitude in sanitation development, where the Bima people are used to a communal living system that prioritizes togetherness and cooperation (gotong royong)[37].
The majority of the Bima tribe adhere to Islam. They are known as a tribe that adheres to Islamic practices in the southeastern Indonesian archipelago. Even so, they still believe in ancestral spirits [37], so this also explains the existence of traditional factors that influence construction or sanitation behavior such as the need for traditional ceremonies, as shown in Table 8.
Feelings (Comfort and Unpleasant Feeling) in the Latrine Usage
A diagram of sanitation practices in the research locations is shown in Figure 4 and tells the tendency of respondents who have private latrines, under certain circumstances, can still practice open defecation. This will be different from the classification based on safe disposal, where the main classification is based on the type of excreta disposal or containment. Monitoring the progress of sanitation uptake could be improved by refining it based on the function of the sanitation system outside the sanitation hierarchy. Inappropriate functioning due to the lack of appropriate usage, cleaning, and access mean that open defecation practices may still occur [38].
The things that influence the use of a latrine from an individual viewpoint is convenience (comfort and discomfort) [16]. Apart from water availability, which is affected by the dry season, other reasons for respondents not to use a latrine all the time are queuing (9%) and discomfort (9%). The large number of family members using the latrine causes queues at certain hours, for example in the morning before going to school and work. Meanwhile, the tendency to conduct open defecation is an unpleasant feeling. These feelings can be: unpleasant to use someone else's latrine frequently (75%) and fear of wasting the latrine owner's water (75%). They also have many family members, so they worry that it will be a hassle if they share someone else's latrine (50%).
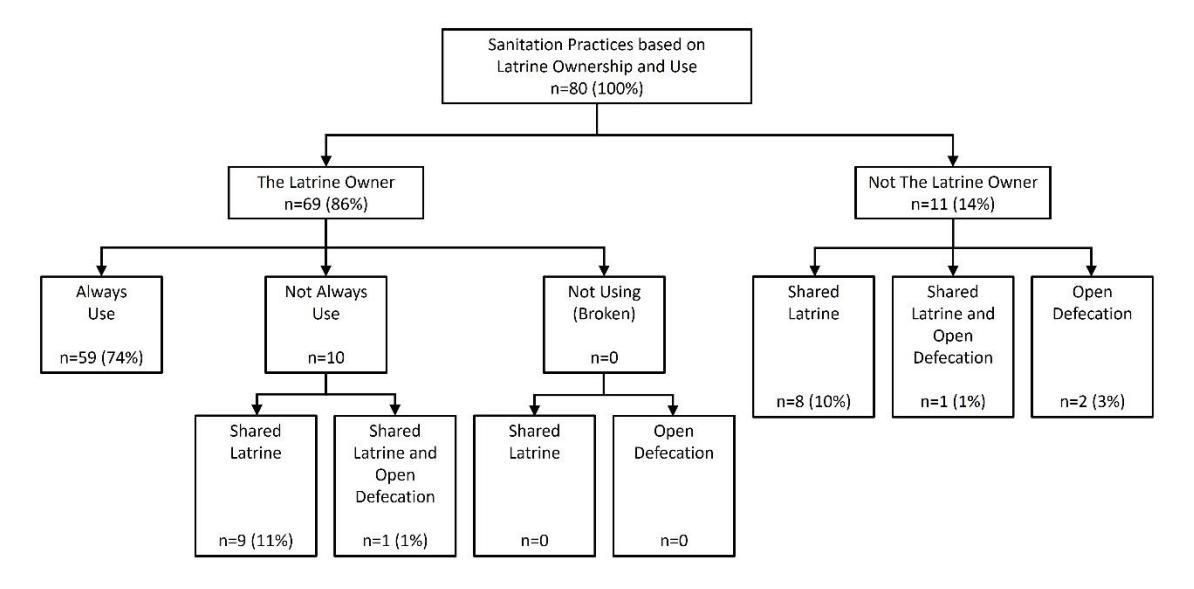
Sanitation practices based on latrine ownership and use.
Knowledge of Safe Disposal
The average knowledge of respondents regarding the risks of domestic wastewater disposed directly into rivers or water bodies and the usage of non-standard septic tanks which can pollute the groundwater and rivers, affecting human health is 3.19. That means the range is 'neutral/normal' to 'agree'. The Mann Whitney U test did not show any significance between latrine owners and non-latrine owners (p-value >0.1). This shows that knowledge about the importance of safe disposal has not been able to influence sanitation behavior in the urban slum areas of Bima City so that there is a gap between knowledge and practice. Therefore, implementing an effective behavior change communication strategy is essential to bridge this gap and ensure the application of knowledge into practical actions [39].
34% of respondents know that septic tanks can be full and desludging is needed, while 24% of respondents say that septic tanks cannot be full and another 42% do not know. 34% of respondents who say that a septic tank can be full, do not know after how long a septic tank will be full and requires desludging. This occurs due to the lack of information regarding latrines and the non-functioning of a fecal sludge treatment plant in Bima City [40].
Limitations
While this study cannot generalize the cultural factors identified within these communities to the broader context of Bima's urban slums, its methodology and outcomes offer valuable insights. The study suggests that a thorough examination of socio-cultural aspects, including individual aspects, is crucial for local professionals to make effective sanitation programs for specific communities. Although the specific cultural factors may not be universally applicable, the study's approach and findings can serve as valuable insight when conducting similar investigations in other urban slums.
Conclusion
This research examined individual aspects within the socio-cultural context that impact community sanitation in the urban slums of Bima City. Following the IFSS framework, individual aspects were categorized into five sanitation stages: acceptability, construction, usage, maintenance, and safe disposal. Factors influencing
sanitation development, particularly latrine construction, at each stage from an individual standpoint include perception, experience, financial capacity, feelings, and knowledge about safe disposal. The study revealed a subgroup of respondents who transitioned from open defecation in rivers to constructing private latrines. Perceptions about the comfort of open defecation and latrine use play a role in influencing individuals to adopt a private latrine. Additionally, the experience gained from using shared latrines in public facilities, communal latrines, or within the community influences the decision to build a private latrine, considering the challenges associated with the sustainability and maintenance of communal latrines. In the construction stage, financial constraints, and the construction capabilities of urban slum communities often hinder latrine construction. However, cultural and traditional values (adat) in the Bima community, despite residing in urban slum areas, mitigate these challenges. The cultural concept of cooperation or gotong royong, strengthened by kinship, facilitates collective latrine construction. Monitoring sanitation adoption progress would benefit from refinement based on the sanitation system's function alongside the sanitation hierarchy. Inadequate functionality, stemming from improper use, maintenance, and access, can lead to continued open defecation practices. Notably, knowledge about the significance of safe disposal has not effectively influenced sanitation behavior in Bima City's urban slum area, underscoring the importance of implementing effective behavior change communication strategies.
Acknowledgments
The authors would like to convey their appreciation to the Netherlands Organization for Scientific Research (NWO) and the Ministry of Education, Culture, Research, and Technology (KEMENDIKBUDRISTEK) Indonesia for providing financial support to this study. This study was carried out as a segment of the Resilient Indonesia Slum Envisioned project (RISE). Moreover, the research also obtained support from the Global Sanitation Graduate School (GSGS) program.