
Introduction
Climate change has emerged as a global challenge, impacting various aspects of life over the past few decades. One of its most noticeable effects has been the significant increase in global surface temperatures up to 1.5 °C (Cai et al., 2022). Increases in the global surface temperature and atmospheric humidity can result in heat stress (Guo et al., 2016) , which has implications for human performance and health (Sylla et al., 2018). When engaging in physical activity in hot and humid environments, the human body plays a significant role in maintaining body heat balance by dissipating heat through radiation, convection, and evaporation. However, these mechanisms are often insufficient because heat production exceeds heat dissipation (Choo et al., 2018). Prolonged exposure to excessive heat stress in hot and humid environments can significantly increase heat strain, potentially impairing work performance (Wittbrodt et al., 2018; Yi and Chan, 2017) and increasing the risk of accidents (Sheng et al., 2018).
This issue is particularly relevant in occupational settings where workers, such as those in agriculture (Rezaei-Hachesu et al., 2022), construction (Acharya et al., 2018), and manufacturing (Pogačar et al., 2018; Seng et al., 2018), are often exposed to high temperatures and humidity while performing physically demanding tasks. These conditions place significant strain on workers' thermoregulation, and failure to manage heat effectively can lead to reduced performance, increased accident risks, and long-term health issues (Flouris et al., 2018). Physical fitness, habits, workload intensity of workers, and environmental factors, such as temperature and humidity, all play key roles in how heat stress impacts performance in occupational settings. Addressing these factors using practical cooling strategies is critical to improving worker safety and productivity.
Numerous studies have suggested various techniques to prevent the increase in heat strain during physical activities in hot environments using body-cooling methods (Shirish et al., 2016; Tokizawa et al., 2014) . These techniques include precooling (Takeshima et al., 2017; Tokizawa et al., 2014) and postactivity cooling (Iwata et al., 2021; Wijayanto et al., 2021) . Precooling is a popular strategy for preventing hyperthermia during physical activities in hot environments. The idea behind this approach is that reducing the core temperature before an activity may increase the heat-storage capacity, delay hyperthermia-induced fatigue, and prevent critically high core temperatures (Ross et al., 2013) . Athletes often use this method in sports science to reduce physiological and perceptual strain in hot environments (Ross et al., 2013; Tyler et al., 2015). However, despite its proven benefits in sports science, its practical application in occupational settings remains limited owing to logistical challenges, such as time constraints, limited access to equipment, and varying physical demands in industrial environments. The potential benefits for worker safety and performance make this an important area for further investigation.
External and internal cooling are common precooling methods used to reduce body temperature during a physical activity. External cooling methods include the use of phase-change cooling vests (PCV) (Gao et al., 2011; House et al., 2013), whereas internal methods include the consumption of ice slurry or crushed ice (ICE) and cold-water ingestion (Wijayanto et al., 2019; Yeo et al., 2012). External cooling methods cool muscle tissues, leading to a more significant decrease in rectal, muscle, and skin temperatures during physical activities (Gao et al., 2011; House et al., 2013). In contrast, internal cooling reduces the temperature of the body's core without affecting the skin temperature (Siegel & Laursen, 2012).
PCV can effectively cool the body by functioning as a medium for storing thermal energy. As the phase-change material transitions from solid to liquid, it absorbs energy (Reinertsen et al., 2008). Studies have shown that PCVs can decrease end-core temperature by approximately 0.2 °C and trunk temperature by 8 °C. Moreover, PCVs can enhance thermal sensation from "hot" to "warm" (House et al., 2013; Reinertsen et al., 2008). However, there is limited research on the effectiveness of PCV cooling in real-world occupational settings, where workers often experience long durations of physical exertion in high-heat environments.
ICE cooling, an internal cooling method, has been suggested as an effective way to reduce heat stress in athletes (Siegel and Laursen, 2012; Yeo et al., 2012). ICE cooling has a high heat storage capacity because it requires additional energy (334 kJ kg) to melt the ice, resulting in a greater heat sink than liquid water alone (Siegel and Laursen, 2012). Earlier studies have found that consuming the slurry before performing an exercise can decrease the core body temperature by an average of 0.32–0.66 ℃ (Siegel et al., 2012; Siegel and Laursen, 2012; Wijayanto et al., 2019). Although research has been conducted on the effectiveness of ICE cooling in athletes, there is a gap in the literature regarding its use in occupational settings. Because many workers perform physically demanding tasks in hot environments, applying ICE cooling in such settings might mitigate heat-related health risks, reduce heat-induced fatigue, and improve overall work performance.
This study investigated the effects of using PCVs for external cooling and internal cooling equipment (ICE) for internal cooling on the physiological and perceptual strains experienced during a physical activity while wearing coveralls in a hot environment. This study compared the differences in physiological strains, such as core body temperature and heart rate, and perceptual strains during physical activities in a hot and humid environment after precooling using PCV or ICE cooling, with those of a no-cooling control condition. By exploring these cooling strategies in a controlled setting, this study aimed to bridge the gap between the well-established benefits of cooling in sports and its applications in occupational environments. The findings of this study can promote workplace cooling interventions that enhance worker safety, thermal comfort, and performance in industries where heat stress is a common challenge. Two experiments were conducted to achieve this goal. The first experiment employed PCV as a precooling method before the participants performed simulated work on a treadmill wearing a working coverall in a hot and humid environment. The second experiment used crushed ice (ICE) as a precooling method before conducting a physical activity under the same environmental conditions. These two methods were evaluated separately owing to their different cooling mechanisms. PCV primarily targets external cooling by reducing the temperature of the skin and muscles, whereas ICE focuses on internal cooling, which directly lowers the core body temperature. The efficacy of the cooling methods applied in these two experiments was evaluated based on the effects of the PCV and ICE cooling methods on physiological and perceptual strains during physical activity and recovery.
Materials and Methods
Participants
Experiment 1 recruited 11 male students with a mean age of 20.8 (±0.2) years, body mass of 70.8 (±4.2) kg, height of 171.1 (±0.9) cm, body surface area of 1.8 (±0.1) m², and maximum heart rate (HRmax) of 187 (±4) bpm. In Experiment 2, nine male students participated, with a mean age of 22.11 (±0.93) years, body mass of 70.78 (±4.24) kg, height of 169.78 (±3.11) cm, body surface area of 1.8 (±0.1) m², and HRmax of 189 (±12) bpm. There were no significant differences in the age or physical characteristics of the participants between Experiments 1 and 2. All the participants were accustomed to running 4–5 days per week, indicating high levels of regular physical activity. Moreover, they were acclimatized to exercise under hot conditions, ensuring that they were well prepared for physical activities in a hot environment. A priori power analysis using the data from Wijayanto et al. (2021) for the PCV experiment with an effects size of 0.57, significance level of 0.05, and statistical power (1-ß) of 0.8 yielded the minimum sample of nine participants. For the ICE experiment, using data from our previous ICE study (Wijayanto et al., 2019) with an effect size of 0.6, significance level of 0.05, and statistical power of 0.8 resulted in a minimum sample of seven participants. Thus, eleven participants in Experiment 1 (PCV experiment) and nine participants in the ICE experiment were sufficient.
Experimental Procedures
Experiment 1: PCV cooling
The participants were required to participate in two experiments in random order on separate days: control condition (CON) and PCV cooling. In the PCV condition, each participant wore a cooling vest containing seven PCM packs with a melting point of 24 °C and a latent heat fusion of 185 kJ kg-1 before wearing the Nomex IIIA coverall. In the CON condition, each participant wore the same experimental clothing as in the PCV condition, but without the cooling vest. The participants wore experimental clothing, including a cotton T-shirt, briefs, shorts, a cooling vest, a Nomex IIIA coverall, socks, and safety shoes.
Upon arrival at the laboratory, the participants were given 250 mL of mineral water to remain hydrated. They were then asked to rest for 30 min to stabilize their physical condition. Afterward, participants wore a Polar HR monitor strap (Polar H7, Polar Electro, Finland) on their chest and a Polar sports watch (Polar A300, Polar Electro, Finland) on their left wrist to record their HR. After attaching the sensors, the participants wore experimental clothing depending on the assigned condition.
Experiments were conducted in two chambers under controlled environmental conditions. The first chamber, where participants underwent a 10-min baseline phase, was set at 28.7 ± 0.4 °C air temperature (Tair) and 50.8 ± 3.5% relative humidity (r.h.) and maintained at a thermoneutral level using an air conditioner. The second chamber, where participants performed a 30-min physical activity, was maintained at Tair of 33.0 ± 0.8 ºC and 72 ± 6% r.h., with the temperature and humidity controlled using an air conditioner with a heating function and a dehumidifier, respectively. The chambers were adjacent, with a door separating them, to ensure a minimal transition time between environmental conditions. During the physical activity phase, participants walked on a treadmill, with the speed set at 4.8 ± 0.3 km/h and the inclination at 1.5 ± 0.5%, adjusted to maintain an intensity corresponding to 65% of the predetermined HRmax. The treadmill speed was started at 2.7 km/h with an inclination of 0%, and both parameters were gradually increased to the target values within 2 min and maintained for the remainder of the exercise. The experiment was concluded with a 20-min recovery phase. The participants wore the PCV throughout all phases under the PCV condition. The experimental protocol is illustrated in Figure 1.
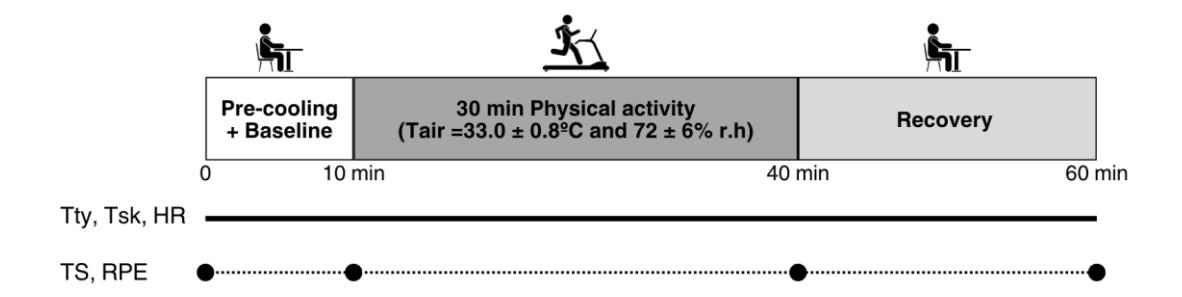
Experimental protocol for the PCV experiment. Tympanic temperature (Tty), skin temperatures (Tsk), and heart rate (HR) were continuously measured during the experimental phase. Thermal sensation (TS) and rating of perceived exertion (RPE) were measured at the baseline (before wearing the PCV), preactivity, end of activity, and after recovery.
Experiment 2: ICE cooling
The participants were randomly assigned to two different experimental conditions, CON and ICE, on separate days. Under the CON condition, participants were given only room-temperature mineral water (25 ℃), whereas in the ICE condition, they were provided with crushed ice made of isotonic water (−2 ℃). The amount of mineral water or crushed ice provided was 7.5 g/kg body mass, as suggested by Siegel and Laursen (2012). The participants wore experimental clothing as in Experiment 1, but without a cooling vest.
Upon arrival at the laboratory, the participants underwent the same instrumentation procedures to attach the sensors. Subsequently, they were asked to wear the experimental clothing. The participants were then asked to cool their bodies for 20 min by ingesting mineral water for the CON condition or crushed ice for the ICE condition. Next, they underwent an experimental session consisting of a 10-min baseline phase in a room maintained at Tair of 28.7 ± 0.4 ℃ and 50.8 ± 3.2% r.h., followed by a 30-min physical activity phase in another room maintained at Tair of 33.0 ± 0.5 ℃ and 73 ± 6% r.h. The physical activity was the same as in Experiment 1, with the treadmill speed set at 4.7 ± 0.7 km/h and inclination at 1.5 ± 0.5% to achieve a workload equal to 65% of the predetermined HRmax. Finally, the physical activity was concluded with a 20-min recovery phase. A summary of the experimental protocol is shown in Figure 2. The experiment was conducted in the same chambers used in Experiment 1.
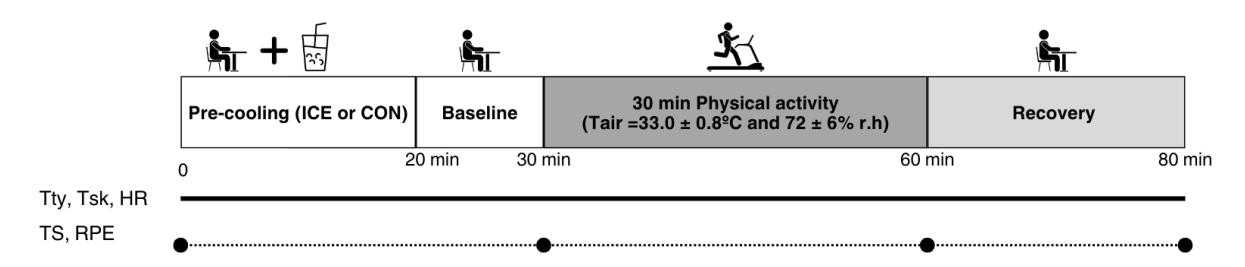
Experimental protocol for the ICE experiment. Tty, Tsk, and HR were continuously measured during the experimental phase. TS and RPE were measured at the baseline (before ingesting CON or ICE), preactivity, end of activity, and after recovery.
Measurements and calculations
Experiments 1 and 2 measured the same physiological and perceptual parameters. The physiological parameters measured in these experiments were core body temperature, representing the thermoregulatory strain, heart rate (HR), cardiovascular strain, and skin temperature. The core body temperature was continuously monitored using an infrared tympanic temperature sensor (CE Thermo, Nipro Corporation, Japan), which recorded the tympanic temperature (Tty) every second. HR was recorded continuously every second using a Polar HR monitor strap (Polar H7, Polar Electro, Finland) and transmitted to an android-based application for HR monitoring (Polar Beat, Polar Electro, Finland). Skin temperature was measured every 2 s on eight body parts (forehead (FH), chest (CH), back (BK), lower arm (LA), hand (HA), thigh (TH), calf (CA), and foot (FT)) using a thermistor (LT-8A; Gram Corporation, Japan). The mean skin temperature (mean-Tsk) was estimated using the modified Hardy–DuBois formula (Eq. (1)).
\[\text{mean-T}_{\text{sk}} = 0.07T_{FH} + 0.35 \frac{T_{CH} + T_{BK}}{2} + 0.14T_{LA} + 0.05T_{HA} + 0.19T_{TH} + 0.13T_{CA} + 0.07T_{FT}\] (1)
Perceptual parameters measured in these studies were thermal sensation (TS), a seven-point TS scale (ranging from 1 = "cold" to 7 = "hot"), and a rating of perceived exertion (RPE) scale ranging from 6 = "no exertion" to 20 = "maximum effort."
Tty and HR data were averaged and used to estimate the physiological strain index (PSI). The PSI was calculated using the modified PSI formula (Equation 2) suggested by Moran et al. (1998).
\[PSI = 5\frac{(T_{ty-t} - T_{ty-0})}{39.5 - T_{ty-0}} + 5\frac{(HR_t - HR_0)}{180 - HR_0}\] (2)
Tty-0 and Tty-t indicate Tty at the baseline and measurement points, respectively. HR0 and HRt indicate the HR at the baseline and measurement points (end of activity and recovery), respectively. The PSI ranged from 0 to 10, with 0 indicating no heat strain and 10 indicating extremely high strain.
TS and RPE data were used to calculate the perceptual strain index (PeSI). The PeSI was calculated using the PeSI formula modified from Tikuisis et al. (2002) (Equation 3).
\[PeSI = 5\frac{TS_t - 1}{6} + 5\frac{RPE_t - 6}{14} \tag{3}\]
TSt and RPEt represent the values of TS and RPE at the last minutes of physical activity and recovery, respectively.
Ethical considerations
The experimental protocols in this study followed the institutional ethical guidelines and adhered to the Declaration of Helsinki. Participants in Experiments 1 and 2 were fully informed about the procedures, potential benefits, and risks, and they were free to withdraw from the study at any time. Informed consent was obtained from all participants prior to their involvement.
Statistical data analysis
The analysis utilized data from the baseline (average of the first two minutes), preactivity (average of the last two minutes of baseline), end activity (average of the last two minutes of physical activity), and recovery (average of the last two minutes of the recovery period). A two-way repeated measures ANOVA was used to study the interaction between the conditions and time. If the two-way ANOVA showed a significant effect, post-hoc tests with Bonferroni correction were performed simultaneously to identify the differences between CON and PCV in Experiment 1, and between CON and ICE in Experiment 2. A paired t-test was used to compare the PSI and PeSI at the end of activity and recovery. Cohen's effect size (d) was calculated to determine the effect of cooling treatment on PSI and PeSI. Cohen's d was used to compare the efficacy of the two cooling methods. The significance level was set at p < 0.05. Statistical tests were conducted using JASP Statistical Software 0.17.3.
Results
Experiment 1: PCV cooling
Figure 3 presents the mean values of Tty, mean-Tsk, and HR at various time points: baseline (Base), before the activity (Pre), during the activity (Activity), and recovery (Recovery) for both the control (CON) and PCV conditions. As shown in Figure 3(A), after 10 min of precooling with PCV, Tty showed a slight decrease (ΔTty = -0.07 ± 0.03 ℃); however, this difference was not statistically significant between the two conditions (p > 0.05). The PCV condition appeared to moderate the increase in Tty during the activity (p < 0.1). This contributed to a more rapid recovery, as evidenced by the lower Tty during the recovery phase compared to that under the CON condition (p < 0.05). The change in Tty (ΔTty) at the end of the physical activity was not significant between CON (1.36 ± 0.18 ℃) and PCV (1.27 ± 0.16 °C, p = 0.40). However, at the end of the recovery period, ΔTty was significantly lower in PCV (1.32 ± 0.15 ℃) than in CON (1.61 ± 0.17 ℃, p = 0.02). Mean-Tsk significantly decreased after 10 min of precooling with PCV and remained lower throughout the activity and recovery periods than that under the CON condition (p < 0.05), as shown in Figure 3(B).
The HR pattern was almost identical under both conditions (Figure 3(C)), with a slight decrease after cooling (-1 ± 3 bpm and -5 ± 2 bpm for CON and PCV, respectively). Both conditions resulted in a significant increase in HR during the physical activity and a subsequent decrease during recovery. During the physical activity, the PCV condition showed a slightly lower HR (p < 0.1) and a quicker return to near-baseline levels during recovery (p < 0.05). The change in HR (ΔHR) at the end of the physical activity was significantly lower in PCV (63 ± 8 bpm) than in CON (75 ± 6 bpm, p = 0.03). Conversely, at the end of the recovery phase, the difference in ΔHR between PCV (24 ± 4 bpm) and CON (31 ± 6 bpm) was not statistically significant (p = 0.19).
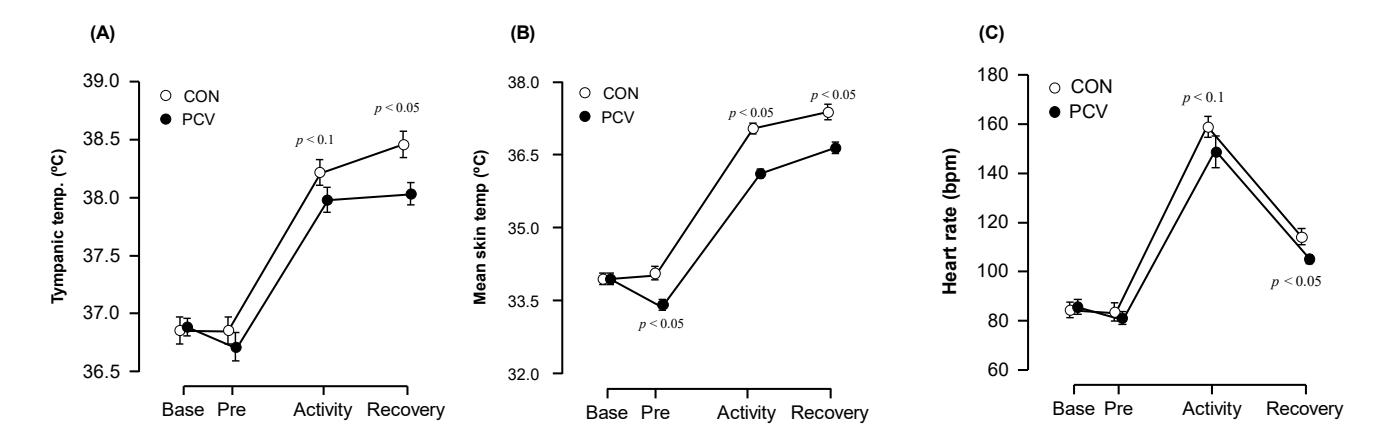
(A) Tympanic temperature, (B) mean skin temperature, and (C) heart rate at the baseline (Base), preactivity (Pre), end of activity, and recovery in control (CON) and PCV cooling.
Figure 4 presents the perceptual parameters, TS and RPE, for the CON and PCV conditions. TS was significantly lower with PCV cooling than with CON, both before and at the end of the activity (p < 0.05). These results indicate that PCV cooling effectively reduces TS during physical activity, as illustrated in Figure 4(A). RPE levels increased at the start of the physical activity and subsequently decreased during the recovery phase, as shown in Figure 4(B). However, the statistical analysis revealed no significant differences in the pattern between the CON and PCV groups (p > 0.05).
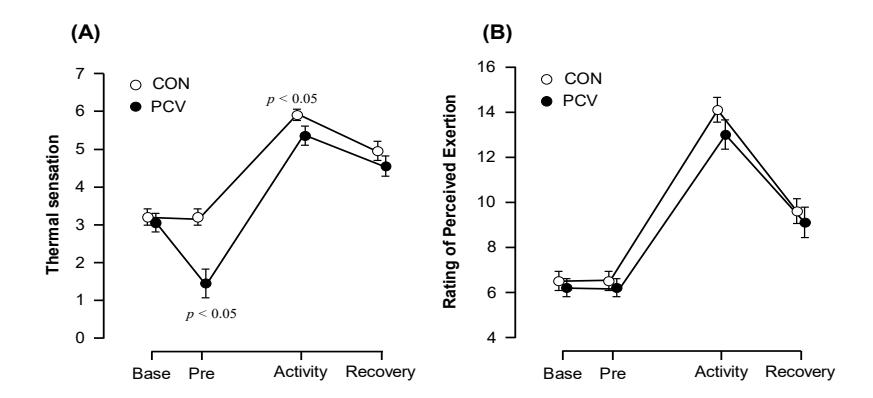
(A) Thermal sensation and (B) rating of perceived exertion at the baseline (Base), preactivity (Pre), end of activity, and during recovery in the control (CON) and PCV cooling groups.
Table 1 lists the PSI and PeSI values at the end of physical activity and recovery under both CON and PCV cooling conditions. The statistical analysis revealed that the PCV cooling condition significantly reduced the PSI compared to the CON condition, both at the end of physical activity (t(9) = 2.39, p = 0.041) and during recovery (t(9) = 3.66, p = 0.005). Specifically, at the end of the physical activity, participants in the PCV cooling condition experienced a medium-to-large reduction in physiological strain (Cohen's d = 0.755). The effect of PCV cooling was more significant at the end of the recovery phase with a large effect size (Cohen's d = 1.157).
Table 1 Physiological and perceptual strain indexes under CON and PCV cooling
| Parameter | CON | PCV | Cohen's d |
|---|---|---|---|
| PSI | |||
| Physical activity | 6.4 ± 0.5 | 5.4 ± 0.5* | 0.755 |
| Recovery | 4.5 ± 0.4 | 3.2 ± 0.3** | 1.157 |
| PeSI | |||
| Physical activity | 6.9 ± 0.3 | 6.1 ± 0.4* | 0.739 |
| Recovery | 4.6 ± 0.3 | 4.1 ± 0.5 | 0.212 |
* indicates a significant difference between the CON and PCV groups at p < 0.05.
** indicates a significant difference between the CON and PCV groups at p < 0.01.
For PeSI, a paired t-test revealed a significant difference between the CON and PCV conditions (t(9) = 2.34, p = 0.044). The effect size was medium (Cohen's d = 0.739), suggesting that PCV cooling significantly reduced perceptual strain at the end of physical activity compared with the control. However, by the end of recovery, the difference between the two conditions was not statistically significant (t(9) = 1.62, p = 0.139), with a small effect size (Cohen's d = 0.514). This implies that any differences in the perceptual strain between the cooling conditions after recovery were less pronounced and not statistically significant.
Experiment 2: ICE Cooling
Figure 5 presents the mean values of Tty and HR at different time points: baseline (Base), before the activity (Pre), during the activity (Activity), and during recovery (Recovery) for the CON and ICE conditions. As shown in Figure 5(A), no significant difference in Tty between CON and ICE conditions at preactivity was observed (p > 0.05). Post-ICE ingestion, Tty slightly decreased (ΔTty = -0.13 ± 0.07℃), whereas under the CON condition, Tty showed a slight increase (ΔTty = +0.12 ± 0.03℃). These changes differed significantly between the two conditions (t(8) = 2.92, p = 0.019). Tty increased during the physical activity, with a significantly lower Tty observed under the ICE condition (p < 0.05). The lower Tty under the ICE condition was maintained throughout the activity and until the end of the recovery period (p < 0.05). At the end of the physical activity, the change in Tty (ΔTty) was significantly lower in ICE (0.97 ± 0.14 ℃) than in CON (1.61 ± 0.08 °C, p = 0.018). Similarly, at the end of the recovery phase, ΔTty remained significantly lower in ICE (0.64 ± 0.12 ℃) than in CON (1.07 ± 0.14 ℃, p = 0.019). There were no significant differences in mean-Tsk throughout the experiment (Figure 5(B)), indicating that no-ICE cooling had a significant effect on mean-Tsk.
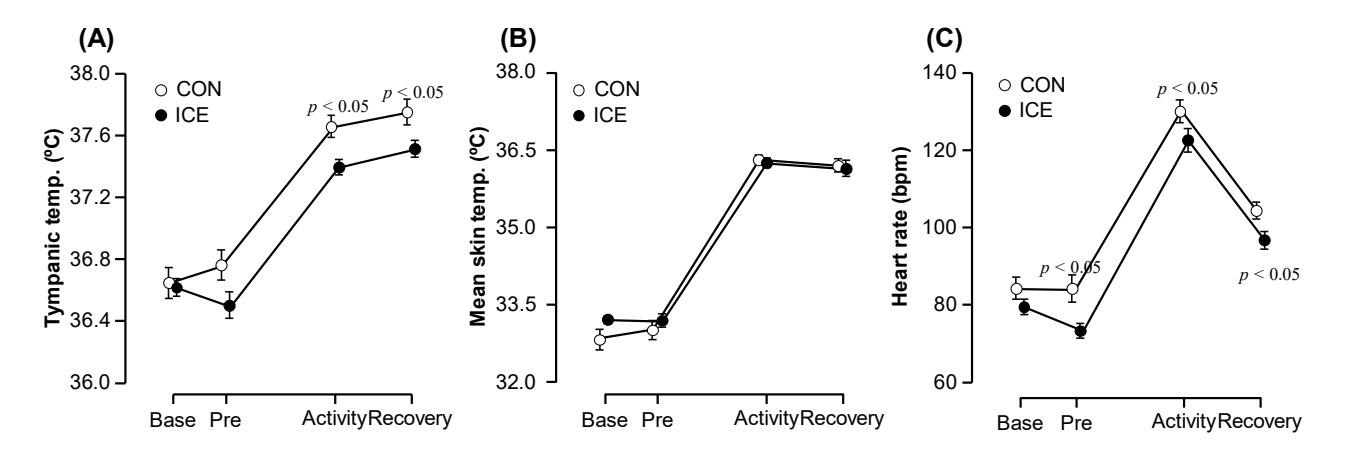
(A) Tympanic temperature, (B) mean skin temperature, and (C) heart rate at the baseline (Base), preactivity (Pre), end of activity, and recovery under CON and ICE cooling.
Following the consumption of ICE, HR decreased significantly and was notably lower than that observed under the CON condition (p < 0.05). Under both conditions, HR increased with the onset of physical activity and then decreased substantially during recovery. At the end of the activity and throughout the recovery period, HR was significantly lower in ICE than in CON (p < 0.05).
Figure 6 shows perceptual parameters TS and RPE for the CON and ICE cooling conditions. The participants perceived TS to be significantly lower under the ICE condition than under the CON condition at various stages: before the activity (preactivity, p = 0.043), at the end of the activity (p = 0.028), and at the end of the recovery period (p = 0.043). For RPE, an observable trend indicates that precooling with ICE may have influenced participants' RPE. Although not statistically significant, RPE was lower underthe ICE condition than underthe CON condition during the preactivity phase (p = 0.051), at the end of the activity (p = 0.074), and at the end of the recovery period (p = 0.084).
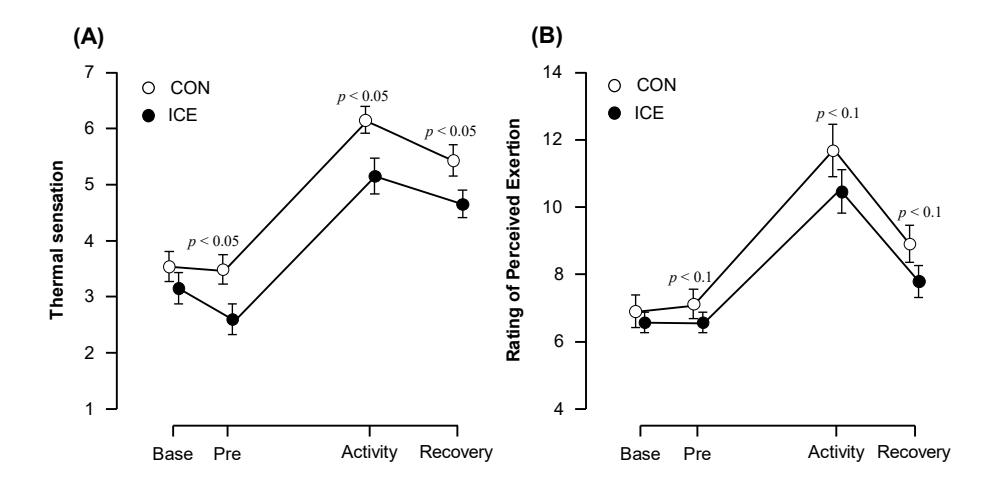
(A) Thermal sensation and (B) rating of perceived exertion at the baseline (Base), preactivity (Pre), end of activity, and recovery under CON and ICE cooling.
Table 2 lists the PSI and PeSI values at the end of physical activity and recovery under the CON and ICE conditions. A paired t-test revealed a significant reduction in PSI for participants who ingested ICE before the activity compared with those subjected to the CON condition at both the end of the activity (t(8) = 3.41, p = 0.009, Cohen's d = 1.135) and during recovery (t(8) = 2.60, p = 0.031, Cohen's d = 0.868). This significant reduction indicates that ICE ingestion is an effective strategy for mitigating physiological strain during physical activities.
As regards the perceptual strain, the trend also showed a lower PeSI for the ICE condition. The paired t-test demonstrated a significant difference between the ICE and CON groups at the end of the activity (t(8) = 3.19, p = 0.013, Cohen's d = 1.065) and recovery period (t(8) = 2.97, p = 0.018, Cohen's d = 0.99). These findings suggest that, in addition to reducing physiological strain, ICE ingestion significantly reduces perceptual strain during and after a physical activity.
| Table 2 | Physiological and perceptual strain indexes under CON and ICE cooling |
|---|
| Parameter | CON | ICE | Cohen's d |
|---|---|---|---|
| PSI | |||
| Physical activity | 4.1 ± 0.3 | 3.5 ± 0.2** | 1.135 |
| Recovery | 2.9 ± 0.4 | 2.4 ± 0.2* | 0.868 |
| PeSI | |||
| Physical activity | 6.3 ± 0.5 | 5.1 ± 0.4* | 1.065 |
| Recovery | 4.7 ± 0.3 | 3.7 ± 0.3* | 0.99 |
* indicates a significant difference between the CON and ICE groups at p < 0.05.
Comparison between PCV and ICE Cooling
On the basis of a comparative analysis of PCV cooling in Experiment 1 and ICE ingestion in Experiment 2 regarding the physiological and perceptual strain indices, our findings reveal distinct outcomes in heat strain management during and after a physical activity. In the PCV experiment, cooling with PCV resulted in a substantial reduction in the PSI immediately after exertion (Cohen's d = 0.755); this significant effect persisted during the recovery phase (Cohen's d = 1.157). This notable decrease in PSI corresponds to a medium reduction in the effect size of PeSI following the activity (Cohen's d = 0.739). However, this marked difference in perceptual strain did not persist into the recovery phase (Cohen's d = 0.514), suggesting a decrease in the effectiveness of PCV cooling over time.
Conversely, in the ICE experiment, ingesting ICE before physical activity led to a significant decrease in PSI both after the activity (Cohen's d = 1.135) and during the recovery period (Cohen's d = 0.868). Similarly, there was a significant difference in PeSI between the ICE and CON conditions after activity (Cohen's d = 1.065) and during recovery (Cohen's d = 0.990). This indicates that the ICE precooling strategy significantly influenced both the physiological strain and subjective experiences of exertion of the participants.
** indicates a significant difference between the CON and ICE groups at p < 0.01.
Discussion
Individuals and workers engaged in physical activities under hot and humid conditions while wearing working coveralls and protective gears may experience elevated physiological and perceptual strains. This study investigated the efficacy of two cooling strategies, that is, PCV and ICE cooling, in mitigating these strains. We observed some physiological and perceptual changes induced by the cooling intervention in both experiments.
The findings revealed that the PCV and ICE cooling interventions successfully reduced the core temperatures. However, the decrease in tympanic temperature before physical activity was more significant in the ICE experiment than in the PCV experiment. Prior studies support this observation, indicating that ICE precooling effectively reduces core temperature, which is typically measured in the rectum. For example, Siegel et al. (2012) documented a temperature reduction of 0.43 ± 0.14 ℃ and 0.66 ± 0.14 ℃ with 7.5 g kg−1 body mass of ICE ingested over 30 min. Similarly, Yeo et al. (2012) reported a decrease of 0.50 ± 0.20 ℃ after consuming 8 g kg−1 body mass of ICE within the same timeframe. In our study, consuming an amount of ICE equivalent to that in Siegel et al. (2012), but over a shorter period of 20 min, resulted in a modest reduction in tympanic temperature (ΔTty = -0.13 ± 0.07 ℃). The moderate decrease in tympanic temperature observed in this study may be attributed to the reduced duration of precooling relative to prior studies, coupled with the methodological variation in using tympanic temperature measurements instead of rectal temperature assessments in preceding research.
In addition to the lower tympanic temperature, we observed that the heart rate was also lower during exercise after ICE ingestion. This feature was observed for the ICE condition, but not for PCV cooling. As suggested by Siegel et al. (2010), the ingestion of ICE is associated with the formation of a heat sink, and thus, effectively cools the core temperature, including the tympanic temperature (Wijayanto et al., 2019). This cooling mechanism allows for a greater capacity for heat storage during exercise, as demonstrated by Tyler et al. (2015), thereby delaying the onset of high internal body temperature. This delayed increase in internal temperature is crucial for maintaining lower tympanic temperatures during a physical activity. Furthermore, the potential heat sink created during crushed-ice ingestion permits the body to produce more metabolic heat without adversely affecting cardiovascular dynamics (Kay et al., 1999). This process leads to an attenuated increase in heart rate, which is supported by studies on the impact of precooling on thermoregulatory responses during exercise (Tyler et al., 2015). Thus, ICE ingestion not only lowers the core temperature but also contributes to a more efficient cardiovascular response during physical exertion, as evidenced by a reduced increase in heart rate.
In contrast to ICE cooling, precooling using PCV for 10 min did not significantly reduce tympanic temperature (ΔTty = - 0.07 ± 0.03 ℃). Similar findings were observed in earlier studies, which reported no difference in core temperature after 15 min (Watkins et al., 2018) or 40 min (Quod et al., 2008) of PCV cooling. This limited effect of PCV on preactivity tympanic temperature could be attributed to its cooling focus on the upper body parts. Rather than lowering the preactivity core temperature, PCV primarily cools the skin on the trunk, as reported in earlier studies (Itani et al., 2016). Lowering the skin temperature without significantly altering the core temperature may increase the thermal gradient between the core and skin, facilitating effective heat loss from the core to the skin (Kay et al., 1999). This process could account for the observation that, despite the limited effectiveness of PCV in reducing core temperature, PCV was successfully controlled the rise in tympanic temperature during physical activities in a hot environment. This suggests that PCV produces cooling effects, as reported in earlier studies (Gao et al., 2010, 2011).
This study found that PCV and ICE interventions before an activity reduced thermal sensation during the physical activity, with the participants experiencing cooler sensations. However, while the effect of PCV lasted until the end of the activity, the impact of ICE cooling extended until the end of the recovery period, indicating a longer-lasting effect of ICE ingestion than that of PCV. This aligns with previous findings that ICE cooling is more effective than PCV cooling in reducing thermal sensations(Watkins et al., 2018), potentially because of the lower body temperature achieved through ICE ingestion (Onitsuka et al., 2015, 2020). Additionally, ICE ingestion was associated with a lower perceived exertion during physical activity, suggesting that its cooling effect might directly influence the perception of effort. This finding is consistent with prior research highlighting the benefits of ICE ingestion in improving the perceived thermal state and exertion in hot and humid environments (Choo et al., 2023). These results underscore the greater efficacy of ICE ingestion than PCV cooling in reducing thermal sensation and perceived exertion during physical activity.
Both PCV and ICE interventions effectively reduce heat strain; however, their impacts differ. PCV cooling diminishes physiological and perceptual strains immediately after exertion but lacks persistence in recovery. Conversely, ICE ingestion consistently decreases physiological and perceptual strain during and after an activity, significantly affecting
physiological strain and subjective exertion experiences. Although both methods mitigate the heat strain, the consistent effectiveness of ICE ingestion throughout physical activity and recovery makes it more advantageous than PCV cooling. In occupational settings, these findings suggest that the PCV and ICE cooling methods have practical applications for workers exposed to hot and humid environments. Although both can be used as precooling strategies before work, the longer-lasting effect of ICE ingestion makes it particularly beneficial for prolonged physical activity. Workers in the construction, agriculture, and manufacturing sectors, who bear high thermal loads and extended work periods, can benefit from incorporating ICE ingestion into their routines to mitigate heat strain more effectively. Furthermore, the practicality of ICE ingestion, given its ease of administration and sustained cooling effects, offers a feasible solution in real-world occupational settings, where long-duration cooling may be required.
This study has several limitations that need to be considered. First, we conducted the experiments separately with two distinct groups of participants. Therefore, we could not directly compare the results between the two groups or draw definitive conclusions. Furthermore, the duration of the experiments was relatively short, and different outcomes may have been observed over an extended duration. Second, these experiments were conducted in a laboratory setting to allow for control of environmental temperature and exercise intensity. However, this controlled environment may not accurately reflect actual work conditions. Third, the cooling periods differed between the two experiments owing to the specific requirements of each cooling method. The ICE experiment required participants to take 15–20 min to ingest the crushed ice, whereas the PCV cooling method, being passive, required a shorter cooling phase. These timing differences were necessary to ensure the effectiveness of each method but may affect direct comparisons between the two interventions. Moreover, the participants in our study were predominantly young students, who might not be a true representative of the working population. Hence, future studies should include more diverse working population samples to improve the external validity of the results.
Conclusion
In conclusion, this study shows that two cooling methods, phase-change vest (PCV) cooling and crushed ice (ICE) ingestion, effectively reduce heat strain during physical activities in work environments. PCV cooling quickly reduces the heat strain, but does not maintain this effect during recovery. In contrast, ICE ingestion effectively reduces heat strain during and after an activity, making it a more effective method, especially in hot and humid work settings. Although PCV is useful in certain situations, ICE ingestion is notable for its longer-lasting impact on physical and perceived exertion. These results indicate that ICE ingestion is a valuable tool for improving workers' health and safety under challenging temperature conditions.
Nomenclature
CON = Control condition
HR = Heart rate
ICE = Crushed-ice condition PCV = Personal cooling vest PeSI = Perceptual strain index PSI = Physiological strain index RPE = Rating of perceived exertion
Tair = Air temperature Tsk = Skin temperature Tty = Tympanic temperature TC = Thermal comfort TS = Thermal sensation
Acknowledgement
Part of this study was supported by a grant from the Domestic Collaboration Research Program of the Directorate of Higher Degree Education, Republic of Indonesia.
Compliance with ethics guidelines
The authors declare that they have no conflict of interest or financial conflicts to disclose.
The experimental protocols in this study followed the institutional ethical guidelines for human subject experiment and adhered to the Declaration of Helsinki.