
Introduction
Maternal health and fetal growth are important factors that require special attention to prepare excellent human resources for the development of a nation. The Indonesian government's efforts to reduce maternal mortality rates and enhance child health outcomes include encouraging a program to improve service facilities at the Community Health Centers. One of the transformations of health services that the government has implemented is procuring ultrasonography devices to monitor the health of pregnant women and fetuses in the Community Health Centers throughout Indonesia. This step is part of the National Strategy for Accelerating Stunting Prevention in 2018-2024, a strategy with priority targets for pregnant and breastfeeding mothers and children aged 0-23 months (Coordinating Ministry for Human Development and Culture, 2019). According to data from the World Health Organization (WHO), medical imaging is needed in clinical situations to establish a diagnosis in 20-30% of cases. In this case, ultrasonography (USG) and simple radiography are sufficient in 80-90% of cases (Recker et al., 2022).
Integrated antenatal care for pregnant women encompasses a series of activities from conception until the comprehensive delivery process begins. The Integrated Antenatal Care Guidelines from the Indonesian Ministry of Health designate ultrasonography as a supporting examination for pregnant women in the first and third trimesters of pregnancy (Ministry of Health of the Republic of Indonesia, 2021a). The gestational sac represents the first indisputable sign identified in early intrauterine pregnancy through ultrasound examination. First-semester ultrasound can be conducted to determine viable intrauterine pregnancy and gestational age and to observe abnormal pregnancy (Doubilet, 2014). As pregnancy continues, ultrasound examination is performed for fetal growth assessments. Fetal biometry, namely crown-rump length (CRL), is used to assess fetal size and estimate gestational age before 14 weeks gestation (Salomon et al., 2019). After 14 weeks, fetal biparietal diameter (BPD), head circumference (HC), abdominal circumference (AC), and femur length (FL) can be utilized to measure the estimated fetal weight (EFW) (Mazaya et al., 2023; Salomon et al., 2019). It is important to continue fetal growth monitoring in third-trimester antenatal care, as routine ultrasonography can detect fetal growth restriction (FGR) associated with small-for-gestational-age (SGA) or large-for-gestational-age (LGA)(Henrichs et al., 2019; Salomon et al., 2019). These conditions can further increase perinatal mortality and morbidity and later become risk factors for degenerative diseases in adulthood (Salomon et al., 2019). The need for appropriate diagnostic tools represents one of the primary keys to achieving the National Strategy for Accelerating Stunting Prevention. Community Health Centers, as first-level health facilities providing diagnostic USG services, play a primary role in routine antenatal examinations for pregnant women and are essential for reducing maternal mortality and the potential for stunting in fetuses and infants. The Indonesian Ministry of Health will gradually meet the need for USG in 10,321 Community Health Centers throughout Indonesia, with a target to be met in 2024 (Kementerian Kesehatan Republik Indonesia, 2022).
Telemedicine constitutes a form of remote healthcare delivery formally regulated in Indonesia through Ministry of Health Regulation No. 20 of 2019 on the Implementation of Telemedicine Services Between Healthcare Facilities (Ministry of Health of the Republic of Indonesia, 2019), Ministerial Decree No. HK.01.07/MENKES/4829/2021 on Guidelines for Telemedicine Services during the COVID-19 Pandemic (Kementerian Kesehatan Republik Indonesia, 2021), and Medical Council Regulation No. 74 of 2020 regarding clinical authority for physicians in providing remote medical services (Indonesian Medical Council (KKI), 2020). These regulations encompass teleradiology, teleelectrocardiography, tele-ultrasonography, teleclinical consultations, and telepharmacy, which may be implemented by hospitals, primary health centers, clinics, and private practices, provided they meet the required standards for infrastructure, human resources, and operational procedures. In Indonesia, telemedicine was initially used primarily for inter-facility consultations; however, during the COVID-19 pandemic, its scope expanded to include remote monitoring of self-isolating patients, remote pharmaceutical services, antenatal care via tele-ultrasound, and chronic disease monitoring for conditions such as diabetes and hypertension (Smith et al., 2020). Similar strategies have been adopted in other countries, driven by technological innovation, healthcare access needs, and global connectivity improvements. Tele-USG is transforming healthcare access, especially in low- and middle-income countries (LMICs), where access to trained sonographers and imaging equipment is limited. It enables remote diagnosis and consultation, thereby reducing costs and improving outcomes. Two main modes of tele-USG are employed: asynchronous and real-time(Dowdy & Harris, 2024).
The USG devices available at the Community Health Centers are basic USG units that still require specialized skills to maximize operational functions and analyze examination result images. Generally, basic USG units provide basic features, such as a convex probe for 2-6 MHz frequency obstetrics and gynecology (OB-GYN) applications, limited digital image storage capabilities, time gain compensation (TGC) that must be set manually, limited image enhancement features, and a battery backup system. Another obstacle is that general practitioners and midwives generally operate basic USG at Community Health Centers. At the same time, while OB-GYN specialists are available only at District Hospitals in limited numbers. To maximize the use of these basic USG units, features that support telemedicine are still needed so that general practitioners and midwives at Community Health Centers can obtain guidance or second opinions from OB-GYN specialists at District Hospitals or higher health facilities quickly and easily.
This study aims to develop an Integrated Add-On Interface Tele-USG for monitoring the health of pregnant women and fetuses at Community Health Centers. This add-on interface will be integrated to upgrade the basic USG features already available at the Community Health Centers to tele-USG capability. The main feature to be developed enables health workers at Community Health Centers to operate basic USG at the bedside for patients while simultaneously transmitting ultrasound images/videos of examination results via real-time streaming. Additionally, a web camera will provide additional information regarding the scanning process on the patient's body to facilitate the mentored diagnosis
process and second opinion delivery remotely by specialist doctors at the District Hospitals or higher health facilities synchronously.
Literature review
The first tele-USG implementation was applied in the aerospace field in the 1960s from the International Space Station through guidance from the Mission Control Center (Sargsyan et al., 2005). The tele-USG system has advantages, including the ability to be applied almost anywhere, making it suitable for reaching remote, underdeveloped, and disaster areas while remaining relatively low-cost. Currently, the tele-USG system has been well-established for examinations in emergency, abdominal, and obstetrics cases by general practitioners in remote areas since the 1990s (Recker et al., 2022).
Innovations in tele-USG with video conferencing in education to train new healthcare workers in remote areas (Boniface et al., 2011; Drake et al., 2021) and in various settings, such as indoor facilities, mountainous terrain, aircraft, and prehospital environments, have showed promising results (Crawford et al., 2012; Smith & Brebner, 2002). The limitations of implementing this technology include the time constraints and patient criticality level (Crawford et al., 2012). However, the challenge is the potential for misinterpretation of images or video data, which can result in misdiagnosis (Recker et al., 2022). Therefore, testing the quality of the images/videos is essential before the tele-USG system is implemented. Interpretation of USG images, including in tele-USG, depends on the quality of image acquisition and operator skills. Several methods have been developed to ensure measurable USG image quality, including qualitative perception-based and standard phantom-based measurements. However, the relatively low-cost, qualitative perception-based measurements utilizing statistics require the involvement of multiple stakeholders, including sonographers, radiologists, and specialist doctors, and are highly susceptible to subjective interpretation by reviewers (Bahner et al., 2011; Metcalfe & Evans, 1992). Conversely, although relatively expensive, phantom-based USG image quality assurance measurements produce more objectively measurable parameters and do not require the involvement of multiple stakeholders as reviewers. In addition, phantom-based measurements can monitor the optimal performance of USG imaging systems and can detect early malfunctions of USG devices (Grazhdani et al., 2018; Hangiandreou et al., 2011; Kollmann et al., 2012).
Several studies have explored the development and implementation of tele-USG systems in Indonesia. An intelligent tele-USG system based on FPGA and mobile platforms was introduced in 2023, capable of real-time data acquisition, feature extraction, and image classification. This system was designed to support healthcare delivery in remote areas with limited medical infrastructure (Jatmiko, 2023). A low-cost image storage system for USG using Raspberry Pi was proposed in 2024, aimed at supporting telemedicine by enabling efficient documentation and transmission of ultrasound images. This approach is especially valuable for primary healthcare facilities in resource-limited settings (Khoirunnisa, 2024).
Indonesia's Ministry of Health, in collaboration with PT Indofarma, launched a telemedicine pilot project (2021–2023) in several Community Health Centers across provinces including Maluku, Sumatera Utara, Jawa Tengah, and Sulawesi Selatan. These facilities were equipped with tele-USG, tele-EKG, and tele-vital sign devices, enabling remote consultations with specialists in urban centers (Jatmiko, 2023). The TEMENIN (Telemedicine Indonesia) app, developed since 2017, supports tele-USG among other services. It was later updated to KOMEN 2.0, aiming to improve e-health literacy and remote diagnostics. However, infrastructure and training gaps still limit its full potential in rural areas (Khoirunnisa, 2024). A policy review conducted by ThinkWell and the Indonesian Ministry of Health (2025) highlighted the need to integrate tele-USG systems into the national telemedicine ecosystem. The review identified key challenges such as financing, regulation, and access disparities, and provided strategic recommendations for sustainable implementation (Mulyadita et al., 2025). In summary, Indonesia is actively piloting tele-USG in rural health centers but faces key challenges in infrastructure, training, and regulation. The proposed system addresses these three key challenges by implementing an add-on to existing basic ultrasound systems, simplifying training for healthcare workers at Community Health Centers through a tele-mentoring system, and initiating regulatory standards for quality assurance of tele-ultrasound imaging by introducing standardized phantom-based testing.
The proposed add-on interface tele-USG will be implemented in Community Health Centers where basic USG devices are generally operated by junior general practitioners and village midwives who require guidance from specialist doctors at higher health facilities. This strategy targets the goal of building a system that requires minimal cost by utilizing existing infrastructure. The proposed system is equipped with software designed to support basic USG so that it can be accessed via a PC that functions as a digital media recorder via a web server. It includes a tele-mentoring feature, enabling healthcare workers at Community Health Centers to consult with specialist doctors at higher-level facilities
regarding patient diagnosis and management. This approach aims to bridge the skill gap among healthcare workers at Community Health Centers, thereby allowing for simplified training.
Another key point is that system performance and image quality testing are carried out using standard quality assurance protocols for two-dimensional B-mode images with standard general-purpose USG phantoms and imaging parameters: depth of penetration, vertical and horizontal geometry, focal zone, and lateral and axial resolution. These image parameters are related to the system's implementation in the early detection of stunting, which is closely related to fetal dimension parameters. This study proposes a standardized phantom-based measurement protocol as an initial effort toward establishing regulatory frameworks for quality assurance in tele-USG services.
Materials and Methods
System Design
The designed tele-USG system represents the implementation of telemedicine, utilizing information and communication technology to enhance basic USG services that are already available in Community Health Centers. This system enables remote USG examinations, allowing obstetrician-gynecologists (OB-GYN) to analyze ultrasound images and videos via real-time streaming. Additionally, the system is equipped with an additional web camera, enabling health workers at Community Health Centers to consult with OB-GYN specialists at district hospitals or other higher facilities during the scanning process. This system facilitates synchronous, mentored diagnosis of USG exams; see Figure 1.
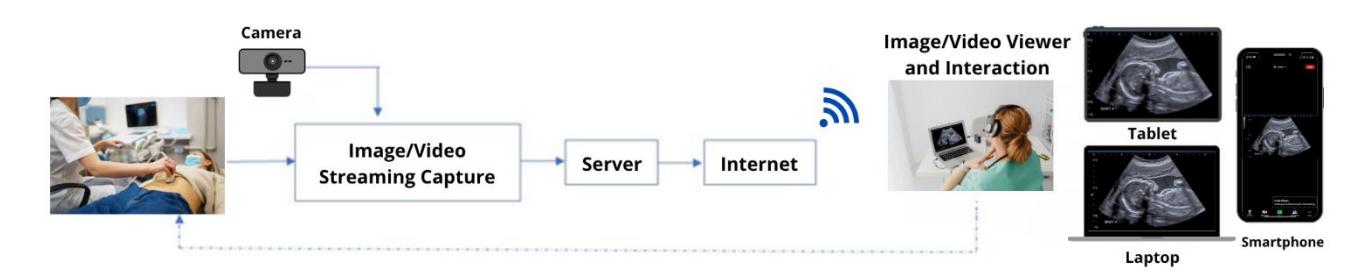
Proposed tele-USG architecture with additional features that allow interaction between health workers in different locations.
In the architecture of the proposed tele-USG, ultrasound images can be transmitted through applications that serve as digital medical record image data. In basic USG systems, most available data communication is based on Digital Imaging and Communications in Medicine (DICOM), which is sent to the Picture Archiving Communication System (PACS) server via peer-to-peer Ethernet cables. The PACS server can be a laptop that stores ultrasound image data to be sent to applications on mobile devices (smartphones or tablets) for medical record documentation. The software flow diagram for the proposed tele-USG architecture is shown in Figure 2. In Figure 2, the process starts by initializing credential information and the database API address to connect to the Firebase database. Users can log in with their registered email addresses and passwords, otherwise, the registration process should be completed. Once logged in with a valid account, the system will proceed with data authentication in the database. If the data are accurate and login is successful, users will access the main interface to record the ultrasound screen or simultaneously participate in a live session. Users can also select the camera device from the main menu on the laptop. Since the tele-USG add-on device is considered a webcam, the external device option should be chosen as the webcam. Thus, users can begin the recording process. Further processes can be performed in parallel to conduct online meetings with medical doctors and other experts or take screenshots of tele-USG results. The stop process allows users to stop the screen recording and obtain a video. Once completed, users are allowed to log out of the system.
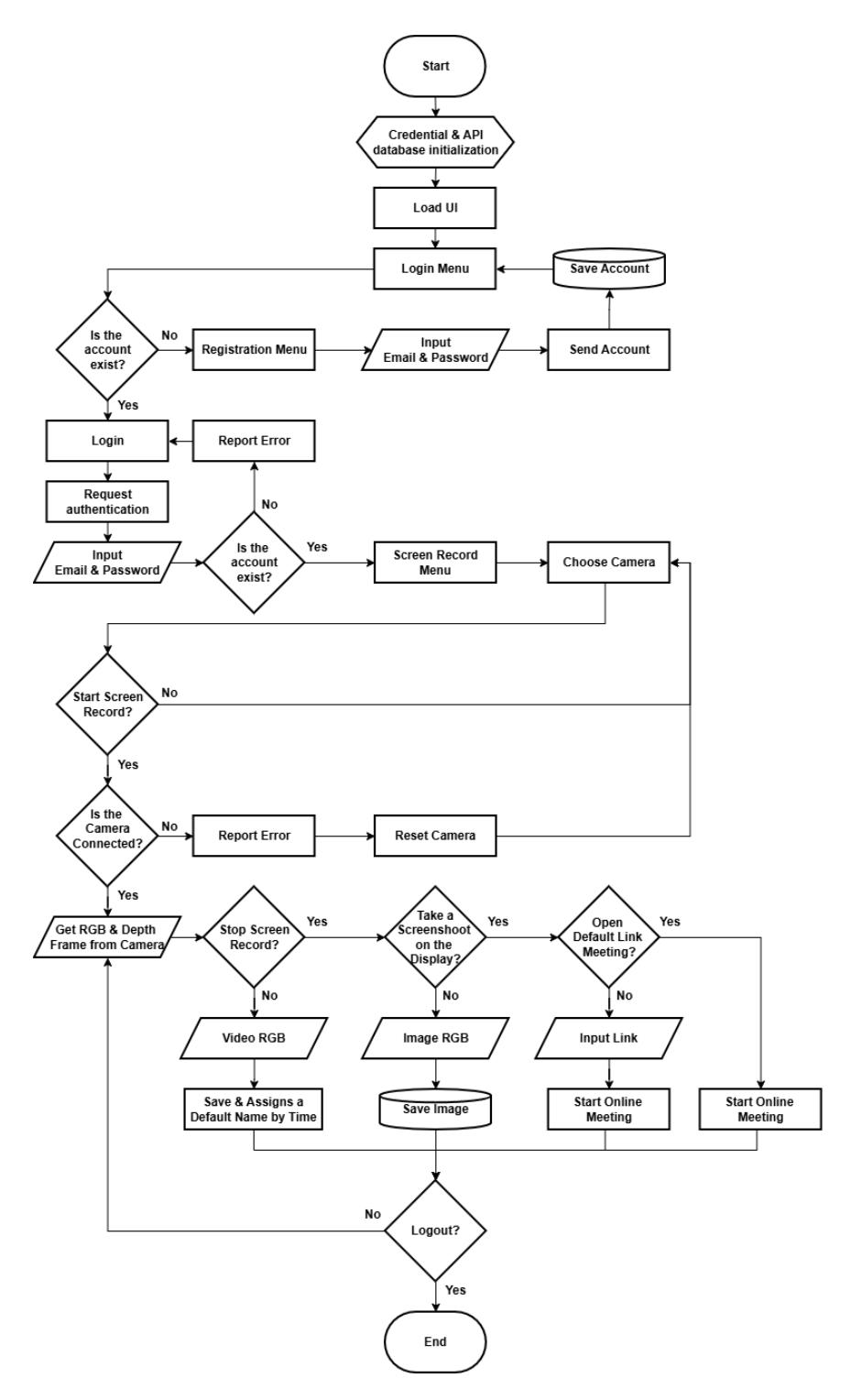
The flowchart of the proposed tele-USG system.
This mentored diagnosis of USG will be carried out synchronously with the addition of a user interface (UI), such as opening a Zoom application link to discuss or share how to use the device. Discussions via the Zoom application can also be stopped at any time with a deactivation decision. This approach can improve accessibility to medical imaging services, particularly in remote areas or locations with limited access to healthcare facilities. Within this framework, the Zoom application serves only as a supplementary communication tool to facilitate direct consultations with experts, rather than as a primary component or a substitute for the system's core functions.
The system itself offers specialized capabilities beyond those of general video conferencing platforms like Zoom, including direct integration with the ultrasound device and structured raw data storage for diagnostic purposes. Furthermore, in future development phases, the system will include a feature for recording diagnostic notes from medical specialists, ensuring comprehensive documentation and supporting continuity of care. Consequently, the Zoom application's role is confined to providing interactive assistance, while all primary diagnostic and data management functions are handled entirely by the system.
The hardware configuration is shown in Figures 3 and Figure 4. The VGA capture device is a modular system that captures and processes analog VGA signals. This system has an integrated cooling mechanism (magnetic fan) to ensure stable performance during operation. The device features a VGA input port to receive video signals from source devices, such as computers or projectors, and a VGA output port for signal pass-through to external monitors. The device incorporates a USB output port for digital signal transfer to a computer or laptop to enhance data acquisition efficiency, enabling seamless integration with video processing software. An audio input port also allows synchronized audio capture alongside video data, ensuring multimedia compatibility. The micro-USB power port is mounted between the top cover and the VGA capture unit and is used to power the fan. This fan acts as an active cooling system to prevent overheating. The casing is designed for durability and to facilitate organized component layout, with dedicated slots for VGA ports, audio ports, and USB ports, optimizing accessibility and connectivity for research and multimedia applications.
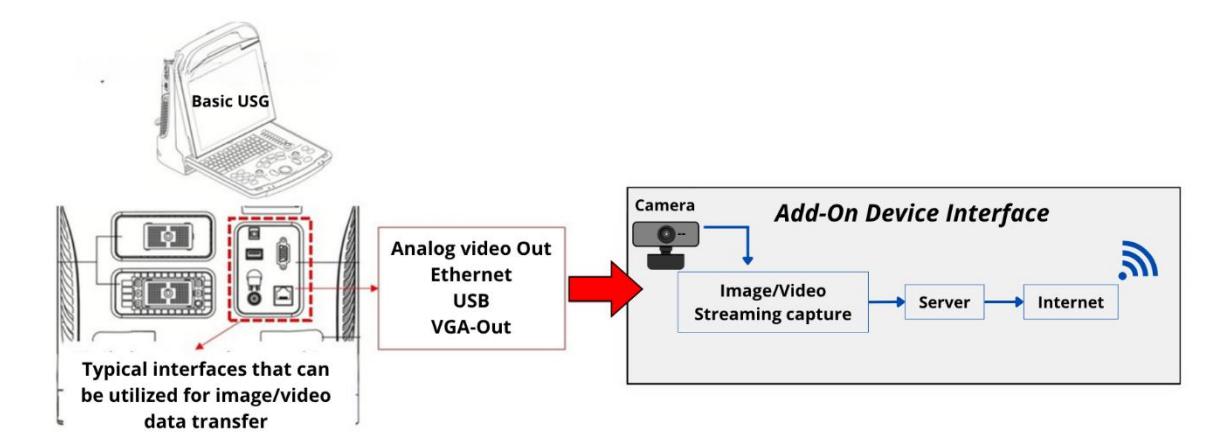
System configuration of the Integrated Add-On Interface tele-USG on basic USG.
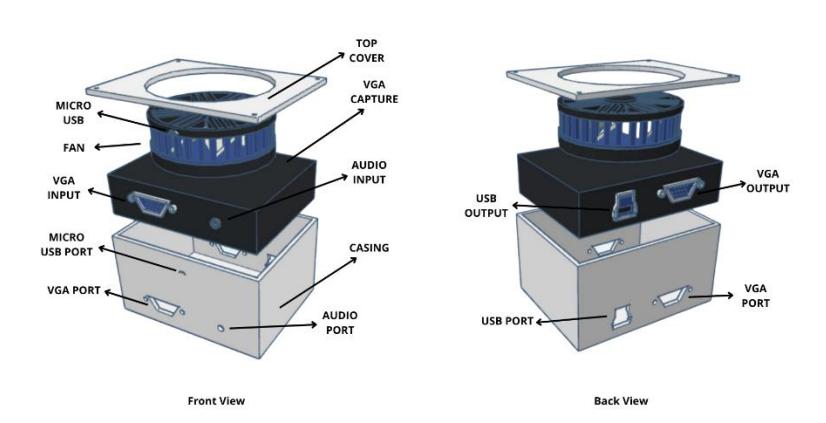
The hardware configuration of the Integrated Add-On Interface tele-USG.
B-Mode Image Quality Assurance Measurement
As mentioned, quality assurance measurement of USG B-mode images is fundamental before the tele-USG system is implemented. Interpretation of B-mode images in tele-USG depends on the quality of image acquisition and operator skills. In this research, phantom-based USG image quality assurance measurements are conducted to monitor the optimal performance of the tele-USG imaging system. B-mode image performance parameters of clinical importance have been developed, including axial and lateral resolution, slice thickness resolution, depth of penetration, contrast resolution, geometric accuracy, focal zone, temporal resolution, and dynamic range (Enriquez & Wu, 2014; Hoskins et al., 2010; Zander et al., 2020). The clinical relevance of those parameters is still debatable case by case. However, all these parameters require a test object that mimics the properties of human tissue. In this research, we tested four parameters directly related to the dimensional features of B-mode images: depth of penetration, geometric accuracy, focal zone, and axial and lateral resolution.
Depth of penetration is the maximum depth at which the echo of ultrasound waves from the scatterer structure can be detected. This maximum depth also refers to the position where the transmitted wave from the transducer begins to lose its energy to be reflected by the scatterers in the form of speckles. This speckle pattern is often difficult to distinguish from the random electronic noise. One way to overcome this is by identifying the last detected speckle pattern point by not freezing the ultrasound image. This is because noise changes from frame to frame, while speckles are constant if the position of the transducer and object do not change (fixed).
Dimensional measurements using ultrasound often involve vertical and horizontal geometric accuracy. The geometric accuracy required in clinical applications varies according to context. For prenatal examination, width measurement requires an accuracy of 1–2 mm (Salomon et al., 2019, 2022), while other measurements can be larger or smaller than that range. Vertical and horizontal distances are quantities used to measure an object's area, volume, depth, and size. Accurate vertical and horizontal distance measurements are essential to support accurate diagnosis. The focal zone or beam profile represents the width profile of the ultrasound wave beam in the lateral direction as a function of depth (axial direction). The shortest horizontal distance measured at a certain depth indicates the focal zone of the wave beam. The best image will be obtained in the area around the focal zone.
An ideal ultrasound imaging system can display a point target as a single point. However, the image of a point target becomes distorted in real imaging systems due to the influence of the infinite bandwidth and the pulse length of the wave, so that it appears as a blurred point or line. Lateral resolution is defined as the ability of an ultrasound device to distinguish (separate) two different target objects that are adjacent in the lateral direction. By comparison, axial resolution is the ability of an ultrasound device to distinguish (separate) two different target objects that are adjacent in the axial direction.
General Purpose Ultrasound Phantom
The test object is required to measure the basic quality assurance of the B-mode images. The key feature is that the test object must have acoustic properties similar to those of human soft tissue: the speed of sound is 1540 m/s, and the attenuation of the material matches that of soft tissue over a wide range of frequencies. These materials are typically aqueous gel or polyurethane rubber equipped with graphite particles, often called tissue-mimicking material (TMM)(Grazhdani et al., 2018; Hoskins et al., 2010). For this research, the four quality assurance parameters of the Bmode images mentioned earlier require a type of general resolution or general-purpose ultrasound phantom CIRS 054 GS shown in Figure 5. This type of phantom typically consists of filaments, pins, and tubes at varying depths of various sizes and impedances (Grazhdani et al., 2018).
CIRS 054 GS general-purpose ultrasound phantom CIRS 054GS
Experiment Setting
The experiment was conducted with a Mindray DP-10 basic USG device with a 75L38EB 5-10 MHz linear transducer. Scanning was performed with a frequency setting of 5 MHz and a dynamic range of 133 and streamed via the Zoom platform. B-mode image quality assurance parameter measurements were performed using the general-purpose phantom CIRS 054 GS, where the transducer surface was treated with standard USG gel. However, future clinical implementation will be carried out on patients with ethical approval.
In Figure 6, it is shown that the host simulates the setting in the Community Health Center consisting of the add-on interface tele-USG (1), which connects the basic USG device (2) and the host laptop (3), which is connected to the internet. A webcam (4) is used to record the scanning process (5). Meanwhile, an additional or guest laptop (6) connected to the internet simulates the setting in the District Hospital or other locations. The host laptop (3) operator and the guest laptop operator are communicating via the Zoom application platform.
The current system implementation remains focused on the fundamental application of tele-USG using ultrasound units of the same type as those used in Community Health Centers and on assessing the extent to which the system can be deployed. Coordination has also been carried out with the national telecommunications provider (PT. Telkom Indonesia) through discussions to evaluate infrastructure readiness in rural contexts. It should be noted that the evaluation in this study focused on image quality assessment rather than network performance testing. For future development, a more comprehensive compression framework will be developed by integrating advanced algorithms optimized for lowbandwidth environments to further minimize file size while maintaining clinically acceptable image fidelity, as recommended in rural telehealth deployment guidelines (WHO, 2022). This enhancement is expected to expand the applicability of the system to underserved rural areas where internet connectivity remains limited.
Experiment setting: (a) simulated setting of the tele-USG system connected via the Zoom platform, (b) the Zoom user interface of the host laptop, (c) the Zoom user interface of the guest laptop
Results
Four parameters were examined: depth of penetration, geometric accuracy, focal zone, and axial and lateral resolution.
Depth of Penetration
The USG device and laptop results show a small difference of 2.74%, with a distortion of 0.24 cm on the laptop. The dimension on the USG monitor is 8.87 cm, while 8.63 cm on the laptop monitor. This dimensional distortion occurs because the discrepancy arises due to differences in screen resolutions between the laptop display (16:9) and the ultrasound monitor (4:3). Therefore, the USG image appears more accurately on the dedicated monitor, while on the laptop screen, the image may appear slightly compressed or stretched horizontally, affecting perceived dimensions.
Geometric Accuracy
In evaluating the geometric accuracy of the tele-USG system, it was observed that five of the eight vertical and six of the seven horizontal targets in the phantom were successfully detected using both the USG device and the laptop. However, differences in geometry are shown in Figure 7 and Table 1. The most significant distortion in the vertical geometry was identified between targets 2 and 3, whereas in the horizontal geometry, the most significant distortion occurred between targets 5 and 6. These findings highlight areas where geometric accuracy is compromised, emphasizing the need for further investigation and potential calibration to improve precision in these regions. These differences may occur due to different monitor resolutions, with each target showing an average of 1 cm distortion. In addition, dimensional differences may also be caused by variations in the resolution of the USG device and laptop monitor used during the Zoom meeting session.
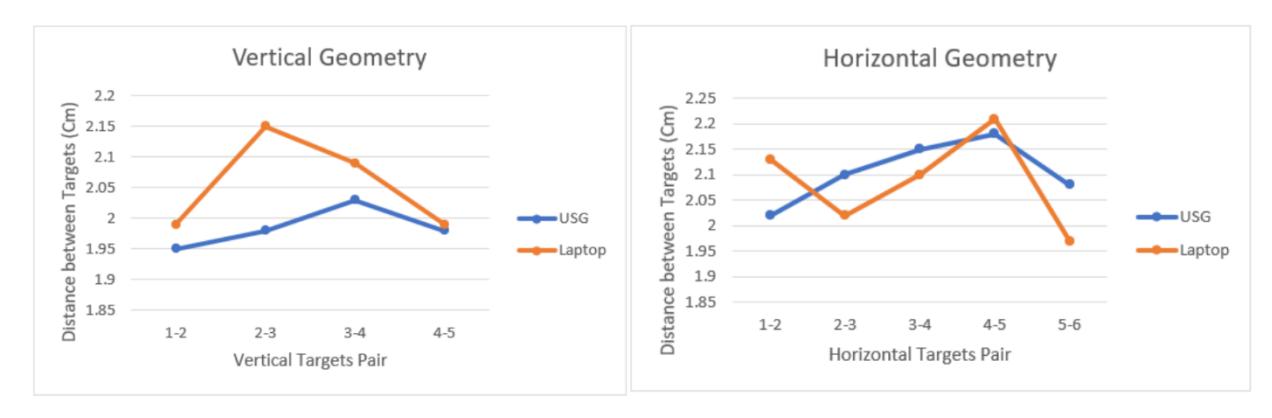
Comparison between the geometric accuracy (vertical and horizontal) between the image on the USG display and on the laptop via the Zoom platform.
Based on the standard deviation calculated using the vertical and horizontal differences in Table 1, the highest standard deviation occurred in target number 2–3 with a score of 0.045, followed by target 1–2 with a score of 0.035, and the lowest was target 3–4 with a score of 0.005. This is consistent with the fact that geometric accuracy still shows a relatively high error—up to 8% or 0.15 cm—which is significant given the very small size of the fetus (approximately 0.5 cm at 4 weeks of gestation).
Table 1 Comparison between the geometric accuracy (vertical and horizontal) between the image on the USG display and the laptop via the Zoom platform.
| Vertical Geometry Distance (cm) | Horizontal Geometry Distance (cm) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Target Number | USG | Laptop | Difference Average % | USG | Laptop | Difference Average | % | |||
| 5 | 5 | 6 | 6 | |||||||
| 1-2 | 1.95 | 1.99 | 0.04 | 1.97 | 2.03 | 2.02 | 2.13 | 0.11 | 2.075 | 5.30 |
| 2-3 | 1.98 | 2.15 | 0.17 | 2.065 8.23 | 2.1 | 2.02 | 0.08 | 2.06 | 3.88 | |
| 3-4 | 2.03 | 2.09 | 0.06 | 2.06 | 2.91 | 2.15 | 2.1 | 0.05 | 2.125 | 2.35 |
| 4-5 | 1.98 | 1.99 | 0.01 | 1.985 0.50 | 2.18 | 2.21 | 0.03 | 2.195 | 1.36 | |
| 5-6 | 2.08 | 1.97 | 0.11 | 2.025 | 5.43 | |||||
Focal Zone
The focal zone measurement was conducted up to the third object on the phantom. The results indicated dimensional differences between measurements taken via USG and Zoom, though these differences were not significant. The smallest variation occurred in the third focal zone, with an average difference of 0.028 mm; see Table 2 and Figure 8.
Table 2 Comparison between the focal zone between the image on the USG display and on the laptop via the Zoom platform.
| Focal Zone Number | USG | Zoom | Difference | Average |
|---|---|---|---|---|
| 0.14 | 0.17 | 0.03 | ||
| 0.17 | 0.19 | 0.02 | ||
| 1 | 0.11 | 0.14 | 0.03 | 0.040 |
| 0.19 | 0.25 | 0.06 | ||
| 0.22 | 0.28 | 0.06 | ||
| 0.17 | 0.17 | 0.00 | ||
| 0.12 | 0.18 | 0.06 | ||
| 2 | 0.14 | 0.14 | 0.00 | 0.036 |
| 0.22 | 0.28 | 0.06 | ||
| 0.25 | 0.31 | 0.06 | ||
| 0.17 | 0.20 | 0.03 | ||
| 0.2 | 0.22 | 0.02 | ||
| 3 | 0.14 | 0.17 | 0.03 | 0.028 |
| 0.22 | 0.25 | 0.03 | ||
| 0.25 | 0.28 | 0.03 |
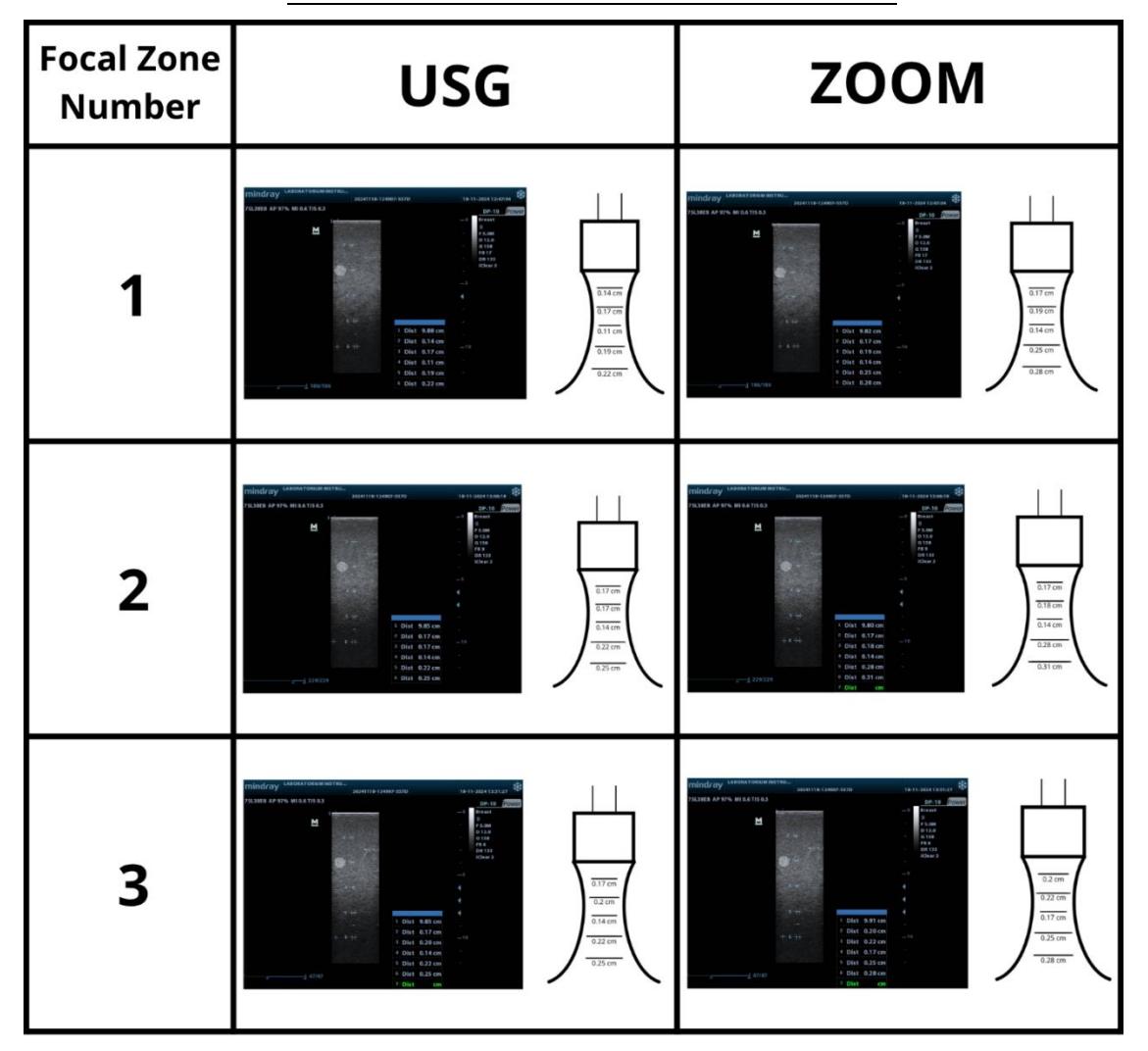
Comparison between the focal zone between the image on the USG display and on the laptop via the Zoom platform.
This minimal difference is attributed to the use of a low-frequency setting, specifically 5 MHz. However, even these small differences are important, as they can impact the measurement of smaller target dimensions within the body. The focal zone plays a crucial role in maximizing image observation efficiency, and improving the signal-to-noise ratio, thereby reducing artifacts and enhancing image clarity. Based on Table 2, the highest overall standard deviation was obtained from measurements using Zoom at 0.058, while that of the USG was 0.047. The highest standard deviation was recorded in focal zone 2 of Zoom (0.074), followed by focal zone 1 of Zoom (0.058) and focal zone 2 of the USG (0.054).
Axial and Lateral Resolution
The finest axial resolution detected is at point A2-B2, with a resolution value between 0.25 and 0.5 mm. Meanwhile, the finest lateral resolution identified is found at point A3-A4, with a resolution value ranging from 1.0 to 2.0 mm. This means that the measurement system demonstrates its highest sensitivity and precision for detecting fine details in the axial direction at points A2-B2, where the resolution is exceptionally fine, allowing it to differentiate features as close as 0.25 mm apart. In contrast, in the lateral direction, the finest resolution is observed at points A3-A4, where it can distinguish details separated by 1.0 to 2.0 mm. These values highlight the system's capability to identify small-scale variations in different orientations.
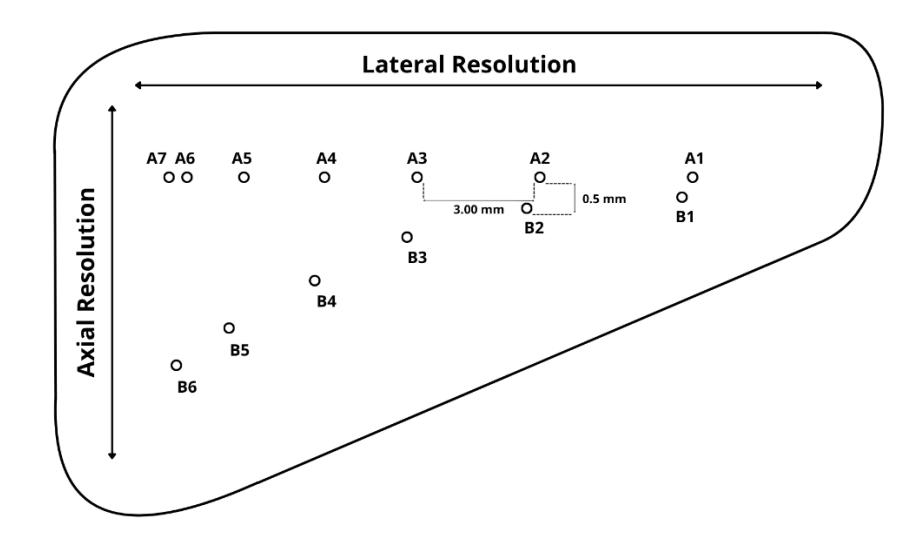
The axial and lateral resolution diagram for general-purpose ultrasound phantom CIRS 054G
Discussions
Depth of Penetration
During the early second trimester, the fetal biparietal diameter (BPD) is typically measured to assess whether fetal growth progresses normally. According to the WHO Fetal Growth Charts, a normal BPD measurement between weeks 14 and 23 of pregnancy ranges from 23-66 mm (Kiserud et al., 2017). If the fetal head diameter is measured as 23 mm on the ultrasound monitor, it may display approximately 22.76 mm on the laptop due to the distortion. This discrepancy could incorrectly suggest a measurement below the normal range.
Furthermore, fetal ultrasound is essential in clinical settings for assessing fetal anatomy, identifying structural abnormalities, and tracking biometric indicators and developmental progress. However, discrepancies in image resolution between ultrasound monitors and standard laptop displays may lead to diagnostic inaccuracies and suboptimal clinical decision-making (Alsaadi et al., 2025). Such inaccuracy in this context may lead to improper prenatal monitoring, such as the misdiagnosis of fetal growth restriction (Wong et al., 2018). Additionally, measurement errors may also stem from the manual placement of the measurement tool (ruler) on the ultrasound image, where the caliper points might not be precisely aligned with the edges of the object. These factors highlight the need for careful measurement techniques and consistent protocols to interpret dimensions accurately.
However, other factors, such as maternal health conditions, can affect fetal biometry measurements and result in deviations from standard fetal growth patterns. For example, gestational diabetes mellitus (GDM) and maternal obesity can significantly increase the ratio of fetal abdominal circumference (AC) to head circumference (HC), increasing the risk by up to threefold (Sovio et al., 2016). In addition, other reports highlight the significance of measuring Crown-Rump
Length (CRL) in fetuses to detect abdominal cysts during the first trimester. Early detection of such cysts may lead to resolution, while in some cases, it can help identify conditions that may result in miscarriages(Passananti et al., 2024).
Geometric Accuracy
The embryonic phase concludes at the end of the 10th week of gestation, during which the crown-rump length (CRL) measures approximately 30 mm. Following this phase, the fetus enters the fetal stage in the 11th and 12th weeks of gestation, during which fetal growth and development can be assessed through parameters such as biparietal diameter (BPD), head circumference (HC), abdominal circumference (AC), and femur length (FL)(Graham, 2010; Mazaya et al., 2023). According to regulations by the Indonesian Ministry of Health, pregnancy ultrasound covered by BPJS (Health Social Security Agency) is conducted once in the first trimester and once in the third trimester (Ministry of Health of the Republic of Indonesia, 2023, 2024). With the results already achieved, geometric accuracy will not significantly affect third-trimester pregnancy examinations. However, to enable comprehensive assessments starting from the first trimester, future system development will include an AI-based image quality enhancer that is planned to be embedded before image data is transmitted via telecommunication networks and received by specialists at higher-level healthcare facilities. This enhancement is expected to reduce geometry-related errors.
Focal Zone
Differences in focal zone placement during ultrasonography in the first and third trimesters of pregnancy can significantly affect diagnostic accuracy, particularly in detecting fetal anomalies and assessing growth (AIUM, 2021; Buijtendijk et al., 2021; Cengiz et al., 2022). The current testing results show an average difference of 0.028 mm, which may affect the diagnosis of fetal anomalies in the early first trimester (under 7 weeks), when the crown-rump length ranges from approximately 0.035 to 0.33 cm (Mayo Clinic, 2025). Fetal size after 7 weeks, up to the third trimester, is generally not significantly affected when the crown-rump length exceeds 1.5 cm. However, this difference can still be improved through the previously mentioned development of an AI-based image enhancer, which is also expected to enhance geometric accuracy.
Axial and Lateral Resolution
Testing of four key quality assurance parameters using standard phantom-based ultrasound imaging—directly related to fetal dimensional evaluation—provides an initial comprehensive overview of tele-ultrasound performance. This serves as a foundation for developing regulations on tele-ultrasound service quality, emphasizing the role of image quality in supporting accurate diagnostic decisions and verifying imaging system performance in line with metrological standards. This initial finding has not been previously reported in the development of similar tele-ultrasound systems in Indonesia. Another key emphasis is on utilizing existing systems by adding hardware and software add-ons to basic ultrasound units, without the need to develop a new system from scratch.
Scalability of the Proposed System
Based on the cost model on Table 3, the proposed tele-ultrasound system can serve approximately 2,000 people at an estimated cost of IDR 7,675 per person per year. With an expected utilization of around 3,000 tele-ultrasound sessions annually, the cost per session is approximately IDR 5,117. By avoiding an estimated 1,200 unnecessary referrals each year, each valued at IDR 50,000 in patient travel and time savings, the system can generate total annual savings of approximately IDR 60,000,000. This results in net savings of approximately IDR 44,650,000 per site per year, corresponding to a return on investment (ROI) of approximately 3.9 times. The break-even point is reached with only approximately 307 avoided referrals per year, underscoring the strong cost-effectiveness and scalability potential of the system for rural healthcare applications.
With this cost model and potential savings, the system can be widely replicated across multiple rural regions without requiring significant additional investment, making it a sustainable and scalable solution for underserved communities. At this stage, the focus remains on system development, with bandwidth testing and detailed assessment of network performance and associated networking costs, particularly for deployment in remote, frontier, and outermost (3T) regions, planned for a subsequent phase.
Table 3 Capital expenditure (CAPEX) and operational expenditure (OPEX) of the proposed system.
| CAPEX | ||||||||
|---|---|---|---|---|---|---|---|---|
| Item | Unit Cost (IDR)QuantityTotal Cost (IDR)Annual Cost (IDR) | Notes | ||||||
| Portable tele-ultrasound device | 15,000,000 | 1 | 15,000,000 | 3,750,000 | 4-year lifespan | |||
| Solar panel & UPS backup | 10,000,000 | 1 | 10,000,000 | 2,500,000 | Ensures operation in low-grid areas | |||
| Network setup & router | 5,000,000 | 1 | 5,000,000 | 1,250,000 | Includes LTE/5G dongle | |||
| Operator training | 3,000,000 | 1 | 3,000,000 | 750,000 | 1–2day session, refresher yearly | |||
| TOTAL CAPEX | 33,000,000 | 8,250,000 | ||||||
| OPEX | ||||||||
| Item | Unit Cost (IDR)QuantityTotal Cost (IDR)Annual Cost (IDR) Notes | |||||||
| Data plan for image transmission | 300,000/month | 1 | 3,600,000 | 3,600,000 | Compressed DICOM/JPEG transfer | |||
| Routine maintenance & consumables2,000,000/year | 1 | 2,000,000 | 2,000,000 | Probe covers, gel, cleaning supplies | ||||
| Remote technical support | 1,500,000/year | 1 | 1,500,000 | 1,500,000 | Online troubleshooting & updates | |||
| Total OPEX | 7,100,000 | 7,100,000 | ||||||
| Grand Total Annual Cost | 33,000,000 | 15,350,000 | Per rural site | |||||
Conclusion
An Integrated Add-On Interface, tele-USG, has been developed to equip basic USGs that are available in Community Health Centers to monitor the health of pregnant women and fetuses. The depth of penetration comparisons between USG devices and laptops show small difference of 2.74%. This dimensional distortion occurs because the discrepancy arises due to differences in screen resolution between the laptop and USG monitors. Additionally, measurement errors may also stem from the manual placement of the measurement tool (ruler) on the ultrasound image.
In evaluating the geometric accuracy of the tele-USG system, five of eight vertical and six of seven horizontal phantom targets were detected using both the USG device and laptop. However, an average distortion of 1 cm was observed, likely due to differences in monitor resolutions between the devices during the Zoom session. The focal zone measurement was conducted up to the third object on the phantom, which showed minor dimensional differences between USG and Zoom readings. The smallest variation (0.028 mm) occurred in the third focal zone, likely due to the 5 MHz low-frequency setting. Despite being minimal, such differences can still affect small target measurements in the body. The axial resolution offers higher sensitivity and precision (0.25 to 0.5 mm) than the lateral resolution (1.0-2.0 mm), enabling the detection of fine details as close as 0.25 mm apart.
Overall, all quality assurance parameters of the USG B-mode images show relatively good results. These results suggest the optimal performance of the proposed tele-USG system in meeting its development objectives to monitor the health of pregnant women and fetuses through closely related dimensional parameters. The proposed tele-ultrasound system is highly cost-effective, offering an ROI of 3.9 times and net annual savings of IDR 44.65 million per site by reducing unnecessary referrals. Its scalability and low per-person cost make it a sustainable solution for rural healthcare, with further development focused on optimizing network performance for remote regions.
Further research and development will address telecommunication quality parameters. In addition, the system will incorporate AI-assisted image processing and enhancement features, implemented on both the host computer prior to data transmission and the receiving computer after data transmission via telecommunication networks. This approach is designed to mitigate the risk of misdiagnosis caused by image and video distortion during long-distance transmission of USG data. Utilizing a lightweight AI model offers two primary benefits: it ensures that transmitted USG data maintain diagnostic accuracy, and it enables system deployment across diverse environments, including areas with limited network infrastructure and basic USG equipment. This efficiency will support the widespread adoption of tele-USG solutions, even in remote regions, emergency scenarios, and mobile healthcare units. Furthermore, the lightweight AI model will facilitate integration into low-power, cost-effective devices, promoting equitable access to digital healthcare services across all segments of society.
Acknowledgement
We acknowledge Telkom University for applied research funding in 2024; Prof. Suprijanto of the Medical Instrumentation Laboratory, Bandung Institute of Technology, for technical recommendations; Ms. Laily Ade Oktaviana, Center of Excellence for Biomedical and Healthcare Technology, Telkom University, for business model calculations; and Moch. Maliki Mulky, student of Computer Engineering, Telkom University, for participating in the experiment and software development.
Compliance with ethics guidelines
The authors declare they have no conflict of interest or financial conflicts to disclose.
This article contains no studies with human or animal subjects performed by authors.