
1 Introduction
Recurrent aphthous stomatitis (RAS) is a common oral mucosal disease, manifesting itself as multiple recurrent round or ovoid ulcers with necrotic centers, yellowish-grey pseudomembranes and well-defined erythematous margins. The prevalence of RAS worldwide varies from 5% to 50% depending on the ethnic and socioeconomic groups studied [1]. RAS is characterized by recurrent and painful ulceration on the non-keratinized oral mucosa, such as the
Received February, 18th, 2020, Revised May 26th, 2020, Accepted for publication October 26th, 2020 Copyright © 2020 Published by ITB Institute for Research and Community Services, ISSN: 2337-5760, DOI: 10.5614/j.math.fund.sci.2020.52.3.3
labial, buccal, and ventral tongue mucosa [2]. The prevalence of RAS was higher in women (57.2%) than in men (48.3%) among professional school students compared to 12 years later when the same subjects had become professional workers [3]. Several factors can induce RAS, including imbalanced nutrition intake and allergic conditions such as atopy [3,4]. Macro and micronutrients are needed for the body. In RAS patients a lack of micronutrients is often found, such as ferritin, folate, or vitamin B12, which is known as a hematinic [5]. It is known that RAS patients can also be atopic or have clinical or latent atopy [6]. Our previous investigation found that there was a correlation between RAS and atopy based on higher serum IgE levels in RAS patients compared to the control group [7].
RAS is an inflammatory disease, where cytokine plays an important role in the immune process. The level of pro-inflammatory cytokines, including IL-6, is raised in RAS [8,9]. Physiological concentrations of IL-6 are relatively low (1-5 pg/mL) in the human serum [10]. The serum level of IL-6 in RAS patients is elevated in response to early indicators of inflammation, which is integral to the immunological host defense [11]. External factors involved in RAS such as food (nutrition) or some allergen in the case of an allergic condition related to RAS can induce oxidative stress, which is involved in several pathological conditions [12]. Oxidative stress occurs when there is an imbalance between the production of reactive oxygen species (ROS) and antioxidants. A previous study has shown that the serum total antioxidant status (TAS) level in RAS patients was significantly decreased, whereas the serum level of nitric oxide (NO) was significantly higher, both compared to healthy individuals [13]. Another study has confirmed a significant elevation of the malondialdehyde level and a significant decrease of glutathione peroxidase activity and of the levels of vitamin E and selenium in RAS [14].
Another condition related to RAS is psychological stress, on which several studies have been carried out. Gallo, et al. used a questionnaire to measure the frequency and intensity of stress symptoms in RAS patients and found higher stress levels in the RAS group than the control group during active episodes [15]. A study on anxienty and depression in RAS patients revealed that their score on the State-Trait Anxiety Inventory-Trait Scale (STAI-T) was higher when compared to the control group [16]. Farmaki, et al. revealed that salivary and serum cortisol concentrations and anxiety levels in RAS patients were significantly higher than in the control group [17]. Stress always leads to decreased immunity, characterized by an increase in glucocorticoid secretion. Stress influences the immune system through two routes: the hypothalamus– pituitary–adrenal (HPA) axis and the autonomic nervous system. Interleukin-6 (IL-6) as an inflammatory cytokine is known to play a role in modulating the
HPA axis response at all three levels: hypothalamus, pituitary gland, and adrenal glands [18].
Although research on IL-6, ROS, and cortisol levels in RAS has been done by previous researchers separately, no studies have been done to link IL-6, ROS, and cortisol in RAS patients. The present study aimed to investigate the differences and correlation between the serum levels of IL-6, reactive oxygen species (ROS), and cortisol in RAS patients with and without atopy.
2 Materials and Methods
A total of 27 subjects were evaluated in this study at the dr. Hasan Sadikin General Hospital, Bandung in August-October 2018. This study was crosssectional and used the consecutive sampling method. The diagnosis of RAS is typically established from history taking and clinical presentation [1]. The inclusion criteria were age between 20-40 years old, male and female, having recurrence of RAS more than twice every year, lack of balanced nutrition based on history taking (lack of vegetable consumption or other imbalanced food intake), low level of routine hematological screening, and a history of atopic disease (atopic dermatitis/allergic rhinitis/bronchial asthma). Exclusion criteria were subjects having severe blood abnormalities based on history taking, oral lesions found such as herpetic stomatitis or traumatic ulcers. This study was approved by the Health Research Ethics Committee of Universitas Padjadjaran with Registry Number 977/UN6.KEP/EC/2018.
After obtaining written informed consent, a 5-ml blood sample was collected from each participant in the morning by a laboratory assistant from the clinical pathology laboratory of Dr. Hasan Sadikin Hospital. IL-6 serum levels were measured using human enzyme-linked immunosorbent assay (ELISA) kit (Elabscience®). ROS serum levels were measured using a human ROS ELISA kit with category number MBS2603394. Cortisol serum levels were assayed by electrochemiluminescence immunoassay (ECLIA) Cobas e 601 (Cortisol No. 11875116 122, Roche).
Statistical analysis was performed using SPSS software, version 18.0 (Chicago, Illinois, USA). The Kolmogorov-Smirnov and Shapiro-Wilk tests were used to test the normality of the data, multivariate analysis (one-way Anova) was carried out to assess the difference between IL-6, ROS, and cortisol levels in the RAS patient group, which was divided into two (with and without atopy), and control. A p-value less than 0.005 was considered statistically significant (See Figure 1).
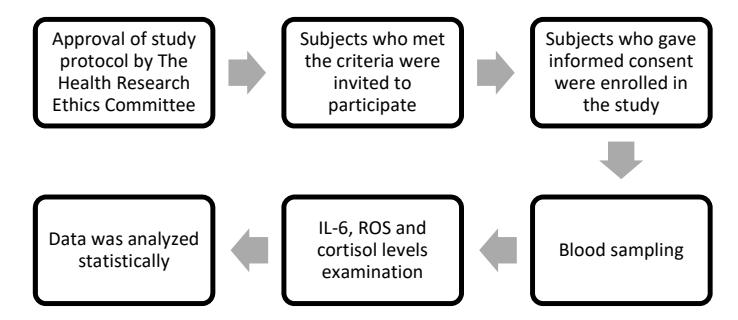
Figure 1 Research flow chart.
3 Results
The RAS patient group consisted of two males and ten females, ranging in age from 21 to 39 years, while the control group consisted of 15 gender- and agematched subjects (three males and twelve females) (Table 1).
| No. | Category | RAS with atopy (n = 8) | RAS without atopy (n = 4) | Control (n = 15) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Age (year) | |||||||||
| 20-30 | 5 | 3 | 10 | |||||||
| >30 | 3 | 1 | 5 | |||||||
| 2 | Sex | |||||||||
| Female | 6 | 4 | 12 | |||||||
| Male | 2 | 0 | 3 | |||||||
| 3 | Atopy | |||||||||
| Allergic Rhinitis (AR) | 3 | 0 | 0 | |||||||
| Atopic Dermatitis (AD) | 3 | 0 | 0 | |||||||
| Bronchial Asthma (BA) | 2 | 0 | 0 | |||||||
Table 1 Characteristics of subjects.
The box plot for the three groups shows a normal distribution (Figures 2-4). The p-value data of IL-6 (pg/ml) and cortisol (nmol/L) were greater than alpha = 5% or 0.229 and 0.849 > 0.05. The IL-6 data (pg/ml) and cortisol (nmol/L) were normally distributed.
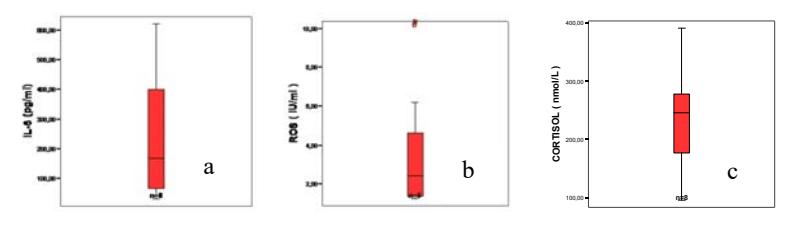
Figure 2 Box plot of RAS with atopy, n = 8 for IL-6 (a), ROS (b) and cortisol levels (c).
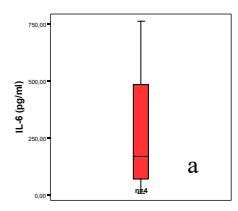
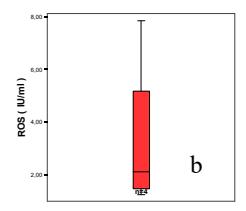
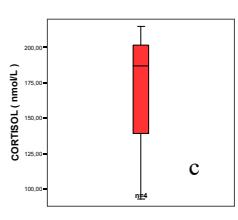
Figure 3 Box plot of RAS without atopy, n = 4 for IL-6 (a), ROS (b) and cortisol levels (c).
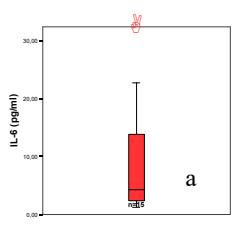
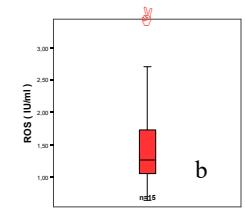
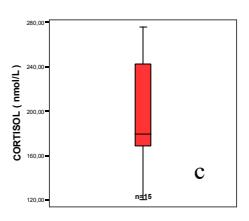
Figure 4 Figure Box plot of control, n = 15 for IL-6 (a), ROS (b) and cortisol levels (c).
Table 2 Normality Test of IL-6, ROS, Cortisol levels.
| Normality Test | RAS ( | with a n = 8) | RAS wit (n | hout at = 4) | topy | Control (n = 15) | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Kolmogorov-Smirnova IL-6 (pg/ml) | Statistic 0.212 | df 8 | Sig. 0.200* | Statistic 0.338 | df 4 | Sig. | Statistic 0.249 | df 15 | Sig. 0.13 | |
| ROS (IU/ml) Cortisol (nmol/L) | 0.307 0.169 | 8 | 0.25 0.200* | 0.353 0.363 | 4 4 | - | 0.229 0.203 | 15 15 | 0.33 0.97 | |
| Shapiro-Wilk | ||||||||||
| IL-6 (pg/ml) | 0.889 | 8 | 0.229 | 0.842 | 4 | 0.201 | 0.839 | 15 | 0.12 | |
| ROS (IU/ml) | 0.77 | 8 | 0.13 | 0.778 | 4 | 0.68 | 0.848 | 15 | 0.16 | |
| Cortisol (nmol/L) | 0.964 | 8 | 0.849 | 0.832 | 4 | 0.174 | 0.931 | 15 | 0.286 | |
* IL-6 and cortisol data show true significance a. Lilliefors significance correction
Based on the results of the normality test (Table 2), the cortisol (nmol/L) and ROS (IU/ml) of the RAS group without atopy were normally distributed. The next test was performed using the Pearson product-moment with r=-0.985 (Table 3). The correlation test showed that there was a very strong relationship between cortisol (nmol/L) and ROS (IU/ml) at an interval of 0.800-1.000 with a negative relationship direction. The p-value obtained was 0.015. When compared with alpha 5%, the value was smaller than alpha, or 0.015 < 0.05, meaning that there was a significant relationship between cortisol (nmol/L) and ROS (IU/ml).
| T . 40 1 | F | RAS and atop | у | R | RAS without atop | ру | Control | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Test of Correlation | r | Strength | p- value | r | Strength | p-value | r | Strength | p-value | |
| Spearman's rank | ||||||||||
| IL-6 and ROS | 0.048 | very weak | 0.911 | _ | - | _ | 0.025 | very weak | 0.93 | |
| IL-6 and Cortisol | - | - | - | - | - | - | -0.036 | very weak | 0.899 | |
| ROS and Cortisol | 0.048 | very weak | 0.911 | - | - | - | 0.429 | moderate | 0.111 | |
| Pearson product- moment | ||||||||||
| IL-6 and ROS | - | - | - | 0.004 | very weak | 0.996 | - | - | - | |
| IL-6 and Cortisol | -0.262 | weak | 0.531 | 0.071 | very weak | 0.929 | - | - | - | |
| ROS and Cortisol | _ | _ | _ | -0.985 | very strong | 0.015 | _ | - | _ | |
Table 3 Correlation analysis between IL-6, ROS, and Cortisol serum levels.
Multivariate analysis for the three groups showed that there was a significant difference between IL-6 (pg/ml) in all groups and a significant difference between ROS (IU/ml) in all groups (Table 4).
Table 4 Difference analysis between IL-6, ROS, and Cortisol levels.
| IL-6 (pg/ml) | ROS (nmol/L) | Cortisol (nmol/L) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Group | n | Min | Max | Mean | Std. Dev | p- value | Min | Max | Mean | Std. Dev | p- value | Min | Max | Mean | Std. Dev | p- value |
| RAS with atopy | 8 | 30,2 | 624,2 | 241 | 213,64 | 1,25 | 10,04 | 3,52 | 3,08 | 95,65 | 391,1 | 236,18 | 91,08 | |||
| RAS without atopy | 4 | 8,5 | 764,2 | 278,57 | 333,77 | 0.000* | 1,23 | 7,84 | 3,31 | 3,07 | 0,049* | 119,8 | 276,3 | 201,05 | 49,55 | 0,239* |
| Control | 15 | 1,2 | 31,2 | 9,51 | 9,29 | - | 0,64 | 3,33 | 1,53 | 0,74 | • | 92,7 | 214,8 | 170,15 | 53,33 | • |
*Multivariate analysis (One Way ANOVA)
4 Discussion
The number of female RAS patients was higher than the number of male patients in this study, as in previous studies [19,20]. In this study we also found that women suffer from RAS and have allergic rhinitis (AR) more often than men, which is consistent with data that AR is often found in women and in the age range of 10-29 years [21]. Allergic rhinitis (AR) is a common disorder of the nose. The symptoms include nasal obstruction, rhinorrhoea, sneezing and nasal itching [22]. In this study, all AR patients who had RAS displayed one or more symptoms.
Four patients in Group 2 were female. One patient said that she always experienced RAS during the menstrual period. Thangadurai, et al. revealed that the onset of RAS is more common during the third week of the menstrual cycle, corresponding the luteal phase [23]. Previous studies have shown that women with menstrual cycle associated aphthae were more likely to have complete or partial remission when receiving therapeutic ovarian hormones; women with menstrual cycle unassociated aphthae were more likely to have no change or exacerbation. These differences were statistically significant (p < 0.001) [24].
Three patients in the RAS group without atopy realized having RAS when under stress due to school exams or other problems. A stressful situation may induce immunoregulatory activity, but the pathophysiologic effects on patients are not uniform. Several previous studies have found a higher level of psychological stress among RAS group patients compared to the control group (p < 0.05) [15]. A more recent study showed that stressful life events were significantly associated with the onset of RAS episodes but not with the duration of the episodes [25]. Stress in RAS patients can elevate serum cortisol levels [26].
ROS levels were higher in one patient in the RAS group without atopy. Based on history taking this patient noticed that the RAS events always coincided with the menstrual period. Menstruation is the periodic, organized shedding of the uterine lining, in response to the interactions of hormones produced by the hypothalamus, pituitary gland, and ovaries [27]. Free radicals are also involved in the reproductive physiology. The ovulatory response is commonly identified with inflammation and reactive oxygen species could be important mediators of those inflammatory reactions [28,29].
Serum IL-6 levels in RAS with atopy were higher than in the other two groups, similar to our previous study on a different population group. It showed that serum IL-6 levels were significantly higher in the atopy with RAS group [30]. Interleukin 6 is a multifunctional cytokine that participates in the inflammatory response [10]. Interleukin 6 gene polymorphisms are also likely to be synergistic for increased IL-6 activity in RAS patients, as identified in a previous study [31]. IL-6 is emerging as an important mediator and novel therapeutic target for chronic inflammatory diseases [32]. Serum levels of IL-6 were found statistically significantly higher in AD patients than in control in [33].
Significant differences in the levels of ROS serum between the three groups can be explained by the presence of more predisposing factors in Group 1 than in the other groups so that free radicals from malnutrition and atopy greatly influenced the increase in ROS levels. A combination of antioxidant-deficiency and malnutrition may render individuals more vulnerable to oxidative stress [34]. All RAS patients experienced mild anemia with a slight decrease in hematological levels due to a lack of nutritional factors [35], especially
micronutrients, because the patients claimed to consume vegetables rarely [36]. Nutritional disorders could also have affected allergic conditions in 8 patients (RAS with atopy) who had a history of atopy. As previous studies have shown, nutrition can modify allergies [37]. The presence of food sensitization and allergies is a predictive of severe atopic dermatitis [38].
Eight patients were in the RAS group with atopy, consisting of three patients RAS with atopic dermatitis (AD), three patients RAS with allergic rhinitis, and two patients RAS with bronchial asthma. Oxidative stress has been known to be implicated in atopic dermatitis for more than 15 years, mainly in the following three aspects: the presence of oxidative stress, increased oxidative stress during AD exacerbation, and decreased antioxidant capability [39]. There is evidence to suggest that an excess of ROS plays an important role in the pathogenesis of airway inflammation in allergic rhinitis [40]. Oxidative stress plays a critical role in the pathogenesis of asthma. It is strongly suggested that an increased level of ROS acts as a critical contributor to the induction of allergic airway inflammation. Oxidative stress has traditionally been considered to be a toxic byproduct of aerobic metabolism and a factor involved in tissue damage [41]. The aphthous process is believed to be initiated by stimulation of the mucosal keratinocytes by a currently unknown antigen, leading to T-lymphocyte stimulation and the liberation of cytokines and various interleukins. As a previous study has shown, oxidative stress plays a vital role in the pathophysiological component of lesion in recurrent aphthous ulceration [42].
5 Conclusion
A significant negative correlation was observed between ROS and cortisol in the RAS group without atopy, and a significant difference between IL-6 and ROS levels was seen in all groups. Collectively, this study suggests that these biomarkers may play a role in the pathophysiology of RAS.
Acknowledgements
The authors would like to thank the referees for their careful reading of the manuscript and their valuable suggestions. This research was partially funded from the Academic Leadership Grant, Universitas Padjadjaran.