
Introduction
Climate change has occurred since three decades ago as a global environmental issue. The connection between the occurrence of diseases and climate factors such as changes in temperature, humidity, and rainfall has been proven, although not directly. Transmission of vector-based diseases such as dengue hemorrhagic fever (DHF), which is spread by the Aedes aegypti mosquito are sensitive to periodic fluctuations in the climate factors (Paul, 2005; Thai and Anders, 2011). In a certain period, the effects of suitable temperature and humidity can increase the reproductive and biting activity of the mosquitoes (Leeson, 1939). Outbreaks of dengue generally occur in tropical regions under strong influences of changes in temperature and precipitation. In 2009, the World Health Organization (WHO) estimated that there are 50 million cases of dengue fever each year, 2.5 million of which occur in vulnerable populations from Aedes aegypti mosquito endemic countries (Bhatt, 2013; WHO, 2009). Indonesia has become one of the largest endemic countries in Southeast Asia. Based on data collected by the United Nations in 2010, Indonesia is the country with the highest number of dengue cases in Asia with as much as 80.065 cases (Sumarmo, 1987; Nair, 2010).
Outbreaks of dengue fever have killed many people, posing a threat to society against vectorbased diseases, especially to those vulnerable to the impacts of climate change. It is necessary to take adaptive measures to anticipate dengue. This includes the adaptation of technology and culture, the provision of adequate health infrastructure, as well as improving the quality of Human Resources (HR) (Rahman, 2012). The vulnerability of society depends on their adaptive capacity in preventing and responding to an increased risk of disease transmission. In efforts to increase resilience to dengue risks, it will be difficult when only relying on increasing the quality of human resources in the health sector. In this context, the overall participation of the community, which is threatened by dengue, becomes significant. Therefore, it is important to increase the capacity of human resources at the community level so they will actively participate in preventing and controlling dengue (Sutherst, 2004; Swaddiwudhipong, 1992).
The United Nations Development Programme (UNDP) defines capacity building as a continuous process involving stakeholders to increase the ability of an individual or organization in effectively, efficiently and sustainably carrying out their functions (UNDP, 1998). Goodman et al. (1998), in their study, explained that the involvement of individuals or groups is important in improving the capacity of the public, one of which is in the field of health. Intervention and active community participation, especially in preserving their surroundings can affect the breeding of the Aedes aegypti mosquito, which carries vector disease (Geana et al, 2013). Nevertheless, still many regions show a lack of active community participation. Capacity building activities are required to improve the capacity and ability of the community, and to be able to overcome problems in the equality of healthcare, monitoring, control, and prevention of dengue vector disease (Labonte, and Laverack, 2001; WHO, 1999).
Transfer of knowledge plays an important role in community capacity building. The knowledge in question may involve ideas and skills needed to improve community capacity in dealing with problems in the neighborhood (Al-Roubaie, 2013). Efforts such as the transfer of knowledge through health campaigns based on education are considered effective in identifying, preventing, and controlling the breeding of the Aedes aegypti mosquito. In addition, efforts to build partnerships and collaborations involving governments, Non-Governmental Organizations (NGOs), as well as the private and public sectors can improve the sustainability of dengue prevention programs in the community (Gómez et al, 2002; WHO, 1999).
Mercy Corps Indonesia (MCI) has carried out a dengue prevention program with an alternative approach based on community participation through the ACTIVE program in Semarang, in cooperation with the government of Semarang (the Health Department, the Regional Development Planning Agency (Bappeda), the Meteorology Climatology and Geophysics Agency (BMKG), the Department of Education) as well as academics of Diponegoro University. The ACTIVE program aims to build a city that is resilient to climate change, especially in the health sector by reducing the incidence of dengue. The program involves several stakeholders in its activities such as the Semarang City Health Department (DKK Semarang), hospitals, public health centers, primary schools, governments at the local level (administrative village and district), as well as the communities in six administrative villages in the city of Semarang. Through the full support of the stakeholders, the ACTIVE Program is considered to show the results of an increase in community capacity, through an alternative approach based on participation.
The alternative approach in the ACTIVE Program is a variation of the method used in a series of capacity building activities such as the use of educational games, a participatory approach, interactive discussions, workshops, the use of modules and props, meetings to mobilize the commitment of stakeholders, adult learning approaches, and mentoring activities that always involve the community. Through this approach, MCI together with the government (Semarang Health Department) was able to increase the community's enthusiasm in participating in various activities ranging from training to practicing the things that they learned related to the control and prevention of dengue in everyday life. In addition to motivating the community, an alternative approach is expected to shape the culture of the community in applying clean and healthy behavior.
Indicators to measure community capacity building can be aspects such as (1) organization, (2) technical issues, (3) community support, (4) a positive perception of citizens of the community, and (5) a sense of belonging and control (Willis and Atkinson, 2005). Studies in Thailand divide the community development model, in particular to the problem of dengue, in three dimensions, namely (1) community-based control and prevention of dengue, (2) the process of community capacity building, and (3) sustainable community-based control and prevention of dengue (C. Suwanbamrung et al, 2011). Concretely, Carmen et al (2005) describe four strategies related to people's behavior in preventing dengue, namely (1) developing community groups to identify priority preventive measures, (2) developing a volunteer group with the sole task of advocating the prevention of dengue, (3) performing home visits as a measure to prevent and control dengue, and (4) conducting a media campaign to support these strategies.
Based on the lessons learned from Suwanbamrung et al (2011) and Carmen et al (2005), this paper aims to assess how an alternative approach based on participation is implemented through the concept of community capacity building within the framework of the ACTIVE Program.
Methodology
This study focuses on observing the efforts of community capacity building with the government through ACTIVE activities conducted by Mercy Corps Indonesia (MCI) in Semarang, in particular in six administrative villages as pilot projects. These include Sukorejo and Sumurrejo in Gunungpati District, Kalipancur in Ngaliyan District, Kramas in Tembalang District, Tlogomulyo in Pedurungan District, and Jatisari in Mijen District. The method used is descriptive analysis with a qualitative approach to study the process of community capacity building. Qualitative descriptive study has the objective to look at case studies comprehensively and is an appropriate method to see the full explanation behind each set of activities (Sandelowski, 2000). By using narrative analysis, the method becomes a major analytical tool for understanding the application of alternative approaches within the framework of increasing community capacity in this ACTIVE program.
Narrative technique is a technique of data collection and analysis that is closely related to qualitative research. Research data is taken from the story/sequence of events based on interviews with respondents. The story is then processed to produce important ideas that can be analyzed. One advantage of using the narrative technique is the emergence of ideas, issues, and problems and as far as until new solutions that come from the story/experience of the respondents. In addition, this method also involves them and makes them become "part" of the study, while the disadvantage is that not all respondents are able to open up in telling their story (Creswell, 2007; Matthews and Ross, 2010). Due to this, important ideas taken from the story cannot be obtained from all respondents. Therefore, it is important to select a number of respondents who can describe the activity intact and in detail.
The collection of data and information was carried out using the interview method with seven respondents who are key informants/champion. The criteria for key informants is that they are representatives/leaders who are chosen and acknowledged by all participants in the activities and are from each of the respective stakeholders of the ACTIVE Program. The key informant is expected to be able to describe the technical processes of the activities in the entire chain of the ACTIVE program and to submit a testimony from the participants of the activities.
The alternative approach used by MCI for community capacity building is an important element in building a society that is resilient in facing dengue. In this study, the researchers observed
how the efforts of community capacity building with the government are carried out using alternative approaches in several activities. The variables used for comparison are based on a study by Suwanbamrung et al, (2011) who considered aspects of sustainable community development, to form three models of community development for facing dengue fever. The models are divided based on the process of community empowerment undertaken to fight dengue. The level of field activities conducted through the ACTIVE program can also be observed through a strategy of Carmen, et al (2005) i.e. to develop community groups and campaign activities to prevent and control dengue fever in the community.
The framework below in Figure 1 explains the phases of the model of community capacity building in facing dengue by Suwanbamrung in Thailand combined with Carmen's strategy, which was carried out by the community in the implementation phase. The model will be adapted as discussion material in examining ACTIVE activities in Semarang.
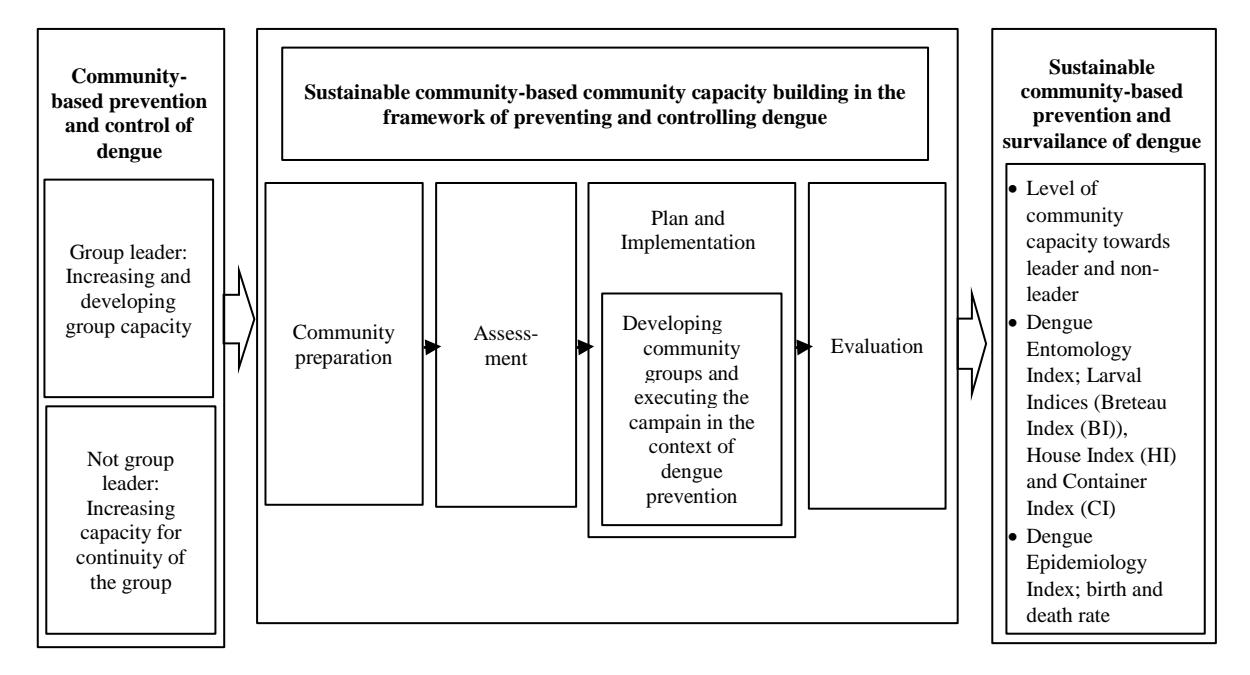
Figure 1. Adaptation of the concept framework of community capacity building in resolving the problem of dengue fever from Suwanbamrung et al, 2011 and Carmen et al, 2005
Results
The ACTIVE program comprises a series of 10 activities in connection with community capacity building efforts. Various methods of alternative approaches are applied in different ways in every activity based on the goals and objectives of stakeholders. The series of activities are divided into three stages, i.e. (1) preparation and training, among others training for trainers (ToT), the community and schools, action orientation group (AOG), training of cadre, empowering small doctors; (2) implementation, i.e. larva monitoring routine (PJR), mosquito breeding site eradication (PSN), the health information system (HIS) and the health early warning system (HEWS); (3) maintaining continuity, through workshops and assistance prior to musrenbang (community discussion about local development needs) and mentoring.
Table 1. Description of ACTIVE activities.
| No | Activity | Description | Method of Capacity Building | Tools and Material | Output |
|---|---|---|---|---|---|
| 1 | TOT (training for trainers) community-based climate change adaptation to face dengue | Training activities of ACTIVE community facilitators | • Training • Games • Interactive discussion • Adult Learning | • Facilitator module • Meta plan • Flipchart • Gimmick | • Producing ACTIVE facilitators to train the cadre • The facilitator becomes an agent of change in the community |
| 2 | Action Orientation Group (AOG) | Forum of socialization and raising of support and commitment of stakeholders towards the ACTIVE Program | • Socialization • Interactive discussion | • Flipchart • Board Marker | • Increasing support and commitment from local actors at the level of administrative village and community unit (RW) • Stakeholders the process of the activities of the Active Program |
| 3 | Trial and simulation of health information system (HIS) and health early warning system (HEWS) | Trial activities to ensure the HIS/HEWS system works well and simulation of implementation using SMS Gateway. | • Presentation • Simulation | • Presentation material • Instructions for HIS/HEWS | • Receiving input from users operating the HIS/HEWS system • Validation and verification of data from users in the 6 pilot project areas |
| 4 | Training for community based climate change adaptation to face dengue | Training to implement the ACTIVE Program for dengue cadre in the community | • Training • Games • Interactive discussion • Adult Learning | • Module • Meta plan • Flipchart • Gimmick | • Increasing community capacity as cadre to implement the ACTIVE program in the general public |
| 5 | TOT school-based climate change adaptation to face dengue | Training activities for ACTIVE facilitators in schools | • Training • Games • Interactive discussion • Adult Learning | • Facilitator module • Meta plan • Flipchart • Gimmick | • Formation of team to support small doctors in implementing the ACTIVE Program in schools • Creating a mechanism for reporting HIS/HEWS system at schools |
| 6 | Empowering small doctors in facing dengue at schools | Activities of training and empowering elementary school students as small doctors in the framework of implementing the ACTIVE Program in the school environment | • Interactive discussion • Games • Training • Children approach | • Module • Meta plan • Flipchart • Gimmick • Props | • Increasing the knowledge and capacities of small doctors as agents of health in controlling dengue disease in the school environment |
| 7 | Implementation of the ACTIVE program in the community and in the school environment | Program implementation through activities of PJR, PSN and health campaigns in the environment of the community by the cadre and at schools by small doctors | House Visit | • Flashlight • larva monitoring routine (PJR) and mosquito breeding site eradication (PSN) report book | • Weekly reports of the results of PJR and PSN inspection • The community receives knowledge so they have the ability to control dengue in the surroundings of their house |
| 8 | Implementation of HIS/HEWS | Applying the method of reporting the results of PJR implementation in the community and school through sending SMS messages to the HIS and HEWS server | SMS Gateway | • Cell phone • PJR and PSN report | • Data regarding Free of Larva Rate (ABJ) and Container Index (CI) • Prediction of dengue events • Early warning system for dengue outbreak • Database information system of dengue cases |
| 9 | Workshop and Pre Musrenbang (community discussion about local development needs) guidance | Socialization, training, and guidance in formulating the community program (particularly health) at Musrenbang on the administrative village level. | • Socialization • Training • Interactive discussion • Guidance | • Musrenbang Form • Flipchart • Metaplan | • Draft of proposed activities to control dengue that will be inserted in the administrative village Musrenbang |
| 10 | Mentoring | Activities of monitoring and evaluation of the implementation of the ACTIVE in the community and at schools | • Interactive discussion • Games • Adult Learning | • Program ACTIVE Implementation report • Gimmick • Metaplan • Flipchart | • Monitoring of ACTIVE program • Evaluation and recommendations as solution for obstacles in ACTIVE activities |
Source: Project Implementation Plan ACTIVE
Stakeholders are actors (individuals or organizations) that have an interest in policymaking and are involved in the process. Stakeholders can usually be grouped by categories: international, public, national politics, commercial/private sector, NGOs, the general public, laborer, and consumers (Schmeer, 1999). The ACTIVE program seeks to create collaboration between stakeholders both at the level of citizens, elementary schools, and government, to jointly increase the resilience of cities by reducing the risk of dengue fever. The Semarang Health Department (DKK) is one of the stakeholders that played a major role in this ACTIVE program. As the highest policy decision maker in the health sector of Semarang, the Health Department is able to mobilize government instruments at the local level, such as public health centers, health survey workers (gasurkes) and cadres of larva monitoring (jumantik) to participate in a series of ACTIVE activities, together with Mercy Corps Indonesia as the NGO who implements activities. The ACTIVE Program is capable of forming a Master of Trainer in charge of transferring skills and knowledge on dengue control activities to the community through a series of training activities using alternative approaches. MCI plays a role in bridging the government of Semarang (DKK) and government at the local level with communities in the areas of the pilot project. In addition, advocacy done by MCI through a participatory approach succeeded in garnering support and commitment of the various stakeholders so that a series of activities could be run by involving stakeholders at all levels. In the implementation process, efforts of community empowerment and cooperation among stakeholders became a key agenda item in each of the ACTIVE activities undertaken with the community.
Table 1 explains the description, the output, as well as the methods used in each ACTIVE activity. In addition, Table 2 explains the alternative approach based on the methods used in carrying out the ACTIVE program. Table 3 describes stakeholder involvement in a series of ACTIVE programs along with the number of participants and the intensity of the activity. The ACTIVE program involves several stakeholders in the process, i.e. government, NGOs, and communities.
Table 2. Description of ACTIVE activities
| No | Method of Capacity Building | Explanation | ||
|---|---|---|---|---|
| 1 | Training | Capacity building of knowledge and ability of participants through explaining the material or direct practical application of the material | ||
| 2 | Socialization | Activities to disseminate information through explaining the material by a source | ||
| 3 | Interactive discussion | Sharing of ideas and information in order to obtain a solution for the issues or problems raised | ||
| 4 | Games | Capacity building of knowledge and ability of the participants packaged in the concept of fun and interactive games | ||
| 5 | Adult Learning | Capacity building of knowledge and the ability through the way of thinking of adults | ||
| 6 | Simulation | Capacity building knowledge and ability through involvement and giving of roles directly to the participants | ||
| 7 | House Visits | Routine Inspection of larva (PJR), Cleaning of mosquito breeding sites (PSN), and a health campaign undertaken by the cadre and small doctors by visiting houses in the community | ||
| 8 | SMS Gateway | Reporting of PJR results by cadre and small doctors via SMS to Health Information System (HIS) and Health Early Warning System (HEWS) server | ||
| 9 | Children approaches | Capacity building of knowledge and ability through the way of thinking of children | ||
| 10 | Guidance | Mercy Corps activities carried out in controlling activities in society, particularly in the implementation of the Administrative Village Musrenbang | ||
Source: Project Implementation Plan ACTIVE
Table 3. ACTIVE Stakeholders
| No | Activity | Personnel in Charge | Involved Stakeholders | Intensity | Participants |
|---|---|---|---|---|---|
| 1 | TOT (training for trainers) community-based climate change adaptation to face dengue | Master Trainer (Staff Mercy Corps Indonesia and 4 representatives of Health Department) | • Public health clinic (Puskesmas) • Health survey workers (Gasurkes) • Work Group IV Family Welfare Guidance in the Administrative Village • Cadres of larva monitoring (Jumantik) | 6 times | 36 participants (becoming facilitator) |
| 2 | Action Orientation Group (AOG) | Mercy Corps Indonesia and Facilitators | • Head of administrative village • Head of Neighborhood Unit (Rukun Warga/RW) and Community Unit (Rukun Tetangga/RT) • Head of the workgroup • Religious leaders • Youth leaders • Community leaders • Head of Family Welfare Guidance | 16 times | 360 participants |
| 3 | Trial and simulation of health information system (HIS) and health early warning system (HEWS) | Mercy Corps and Team from Health Department | HIS/HEWS users: • Regional Technical Implementation Unit (UPTD) • Heads of schools • Teachers of physical education and sports (PJOK • Head of public health clinic • Head of District • Head of Administrative Village • Head of neighborhood unit and community unit | 1 time | 35 participants |
| 4 | Training for community-based climate change adaptation to face dengue | Facilitators (Public health clinic, Health survey workers, District, and Workgroup 4 Administrative villages) | Community (Cadre representation) | 30 times | 319 participants (then becoming cadre) |
| 5 | TOT school-based climate change adaptation to face dengue | Master Trainer (Mercy Corps) | • Staff of Education Department • Regional Technical Implementation Unit (UPTD) Education • Staff of public health clinic • Teachers of physical education and sports (PJOK) | 6 times | 36 participants (then becoming school facilitators) |
| 6 | Empowering small doctors in facing dengue at schools | Facilitators (Teacher) • Regional Technical Implementation Unit for Education • Staff of public health clinic and teachers of physical education and sports (PJOK) | Small doctors | 19 times | 193 participants |
| 7 | Implementation of the ACTIVE program in the community and in the school environment | Cadre and small doctors | • Community in the surrounding of schools | Implementation after training of cadre | All cadre and small doctors |
| 8 | Implementation of HIS/HEWS | Cadre and school teachers | • HIS/HEWS team • Community in the surrounding of schools | Implementation after trial and simulation | All cadre and school teachers |
| 9 | Workshop and Pre- Musrenbang guidance (community discussion about local development needs) | Mercy Corps and Facilitators | • Neighborhood Unit (RT), Community Unit (RW), District, Administrative Village | 1 time | Neighborhood unit (RT), Community unit (RW), District, Administrative Village |
| 10 | Mentoring | Mercy Corps and Facilitators | • Cadre and community | Once every 3 months | All cadre |
Source: Project Implementation Plan ACTIVE
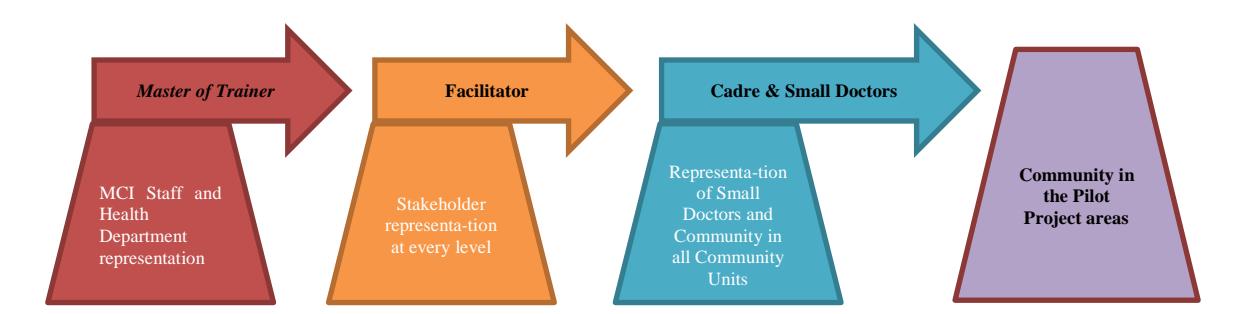
Figure 2. Stages of capacity building (transfer of skills and knowledge) based on the role in the ACTIVE Program
Source: Analysis by Researcher (2016)
Figure 2 illustrates the flow of capacity building through the transfer of skills and knowledge as conducted in accordance with the roles at each level. The process begins with a briefing by the Master of Trainer consisting of two staff of MCI and four representatives of the Health Department. The activity managed to produce 33 community and school facilitators. Community facilitators then train a cadre of representatives of each Community Unit (Rukun Warga/RW); in addition, the school facilitator empowered the small doctors. The cadre was derived from 56 Community Units with 312 actors who implement ACTIVE activities and at the same time provide guidance to the community. Meanwhile, in the school surroundings implementation is carried out by small doctors from 19 schools. Each briefing or training uses the same method, i.e. an alternative approach supported by learning modules. An alternative approach packaged with the use of games, interactive discussions, and adult and children learning can effectively support the transfer of skills and knowledge.
Discussion
Based on the adaptation model of Suwanbamrung et al (2011) and Carmen et al (2005), below is the explanation of the process of ACTIVE activities:
1. Community-based dengue control and prevention
This initial stage involves socialization to all relevant stakeholders of the ACTIVE program that will be carried out, and then the functions and roles are divided through a process of capacity building for both the leader and non-leaders. Leaders will receive training called Trainer for Trainers (TOT) from the Master of Trainer i.e. MCI staff assisted by representatives of the Health Department who will transfer their knowledge and skills to potential facilitators at the community and the primary school level, e.g. representatives of schools, health center officers, district health survey workers (gasurkes), Work Group IV Administrative Village Family Welfare Guidance and Cadres of larva monitoring (Jumantik).
In this training, participants are introduced to participatory training methods that make participants more actively involved in order not to feel bored. Participation can be seen as empowering efforts that involve the community in effectively developing skills and abilities. Therefore, a professional coach is needed that so that transmission of knowledge is in accordance with the procedures (WHO, 1991). The training activities need the attendance of the Master of Trainers who is capable of empowering the community in a participatory way supported by the knowledge and ability to control dengue fever in the community. MCI staff and Semarang City Health Department have these skills. They are able to become a professional
Master of Trainers and successfully produce facilitators that are able to train the community (cadre) in an effort to control dengue. In addition to training the community, TOT is also done in the scope of primary schools using the same method. The success of this training can be seen from the output of activities, which produced 33 facilitators, and from the enthusiasm of the participants in accepting the training materials. Sapto Rini, as TOT participant in the community, explains,
"The training is very different and more interesting than training/education in general. Using participatory methods through games and interactive discussion, TOT participants did not feel bored and were very enthusiastic."
TOT activities are considered successful in forming a team of facilitators and assistants at the administrative village level who have the ability to conduct training and organize activities of prevention and control of dengue fever in the community and the school environment.
After TOT, Action Orientation Group (AOG) are activities of socialization at the same time aiming to garner support and commitment of all stakeholders in the community in order to achieve the purpose of the ACTIVE program. The interesting thing that can be observed is the socialization agenda that is carried out when the ACTIVE program is already under way. Ellen, as the project coordinator, explains
"AOG is a unique and interesting activity. In addition to garnering support, also a socialization process is carried out after the TOT activity of the ACTIVE Program. At this stage, MCI is not an actor leading the AOG discussion, but a facilitator originating from society."
The presence of a facilitator coming society who at the same time is the main actor in leading the Action Orientation Group (AOG) discussion is expected to strengthen the position of the ACTIVE Program, which is very important and needed by the community related to managing the dengue disaster in their region. Building partnerships with stakeholders who have an interest in the neighborhood of residents, especially community leaders, is considered fundamental in initiating community empowerment.
Several countries have shown that communication and social mobilization is effective in the prevention of dengue. The role of community leaders is essential to support community empowerment efforts, so building partnerships is expected to increase the commitment to dengue prevention activities (Parks and Lloyd, 2004). Setio Budi, as community leader, testified that
"The method used in the AOG activities is very interesting because it combines the providing of information with public participation by inviting stakeholders to take action."
In this Action Orientation Group (AOG) activity, the ACTIVE program managed to get the support and commitment of all the community leaders (heads of Neighborhood Units (Rukun Tetangga/RT), heads of Community Units (Rukun Warga/RW), youth activists and religious leaders) in the six of pilot project regions.
The last stage i.e. capacity building for non-leaders, community representatives and small doctors who are responsible for implementing the activities of Larva Monitoring Routine (PJR) and Mosquito Breeding Site Eradication (PSN) in the surroundings of community and schools.
Capacity building is carried out in the form of training using the same method as Trainer for Trainers (TOT), i.e. a participatory method. Alternative approaches used in this training include simulations and educational games. Multimedia tools, games, simulations, and interactive activities are important and interesting learning method in learning about the environment (Nemerow, 1996). Studies in the Philippines by Lennon and Coombs on school students proved that approaches using educational games are quite effective in introducing dengue prevention to children (Lennon and Coombs, 2005). As a school facilitator, Sri said that
"The substance of the material presented is easy to understand for children (little doctors) because it uses interesting props, and the delivery of information happens through games."
Likewise with Mandy as a training participant and cadre who explained
"The participatory methods that are used make the material easy to understand and not monotonous. This is also supported by the available training module."
Training in the community to produce a cadre that is ready to become agents of dengue fever control in society. In the scope of the school, activities are undertaken that will empower small doctors tasked to monitor the existence of larva in their school environment.
2. Community capacity building in order to sustainably control and prevent dengue
This stage comprises the implementation process of training outcomes in the form of campaign activities at homes related to efforts of dengue prevention and control, such as Larva Monitoring Routine (PJR), Mosquito Breeding site Eradication (PSN), until activities systematic reporting using the Health Information System (HIS) and Health Early Warning System (HEWS).
The preparation process of implementing the training results is carried out by the cadre through forums/small-scale meetings. This is done so coordination is maintained in each team in every Community Unit in the pilot project administrative villages. MCI Project assistants still provide assistance as community empowerment and a means of bridging the public and the government in preventing and fighting dengue disaster. Utilization of cadre teams is the same as was done by Carmen et al (2005) to prioritize community involvement through health campaigns, house visits, and discussions as a form of community development in raising public awareness of dengue disaster.
Larvae surveys are conducted regularly by the cadre that followed the Climate Change Adaptation training concerning the Control of Dengue Virus in the community. House visits that are carried out by cadres already include activities of Larva Monitoring Routine (PJR), Mosquito Breeding Site Eradication (PSN) and public health campaigns. Furthermore, reporting the results of monitoring by the cadre to the Health Department is done manually, but uses the SMS Gateway system, which is integrated with HIS and HEWS. After the first training in September 2015, already more than 700 reports were sent to the server or system by 208 people from 58 Community Units in six Administrative Villages in Semarang. At least 319 cadres, community leaders, and residents have been trained in larva monitoring and reporting the jumantik results through SMS Gateway. Based on the last record in February 2016, already more than 8000 reports have been sent to the server.
The same as related to the reporting system can also be seen at 19 schools in the six Program ACTIVE Administrative Villages. After completion of training, then simultaneously once every week the small doctors, accompanied by PJOK teachers (Physical Education, Sport and Health) carry out Larva Monitoring Routine (PJR) activities in the surrounding of schools and in homes in the neighborhood of the school. After the small doctors conduct PJR, written reports are submitted to their tutors (PJOK teachers), and then the tutors report the student's activities to HIS and HEWS via SMS Gateway. Integration between larvae survey with the HIS and HEWS system can be categorized as an alternative approach conceptualized by the ACTIVE Program.
However, various problems also occur during implementation, e.g. apathy among some groups in the community who do not want to receive a house visit by a dengue cadre. In addition, there was also a declining morale of some cadres in the absence of incentives on an ongoing basis, both in facilities and funding. Rimba, as cadre, explained
"The ACTIVE program is generally well received by the community, but some do not agree with a home inspection. I was also concerned with the consistency of PJR and PSN activities by the cadre post ACTIVE mentoring activities by MCI"
3. Sustainable control and prevention of dengue
The last stage is the effort to maintain continuity through monitoring, evaluation, and surveillance of communities and schools so prevention and control of dengue continue to be carried out. According to Government Regulation of the Republic of Indonesia No. 8 Year 2008 Community Discussion on Development Planning, hereinafter abbreviated Musrenbang is a multi-stakeholder forum in the context of regional development plans (Government Regulation Indonesia Year 2008 on Stages, Procedure for Preparation, Control, and Evaluation of the Implementation of the Regional Development Plan). The issue of dengue, which is accommodated for in regional policies, is a form of commitment and surveillance of the government in overcoming dengue in Semarang. Therefore, these policies can be developed into concrete programs in the community and can provide a more comprehensive attention from the various parties.
Workshops and Pre-Musrenbang guidance are carried out as a "tool" to facilitate the government and communities in addressing health issues in Semarang, particularly dengue. Therefore, it becomes a consideration in proposed government programs through Musrenbang to be done by the community.
In addition, activities of mentoring that are carried out are a form of monitoring and evaluating the performance of the cadres in carrying out PJR, PSN as well as in the implementation of reporting via HIS and HEWS. Jabbar, as project coordinator, states
"Mentoring is not a monitoring and evaluation activity in general. However, the element of capacity building through the transfer of skills and new knowledge continues to be carried out, through the method of discussion of solutions and exchange of experiences between groups of cadres"
Mentoring uses the concept of a mentor (MCI staff assisted by a facilitator) and mentee (from cadre) when interacting in this activity. Although it aims to conduct monitoring and evaluation, mentoring activities emphasize capacity building using alternative approaches. The concept of transfer of skills and new experiences is conducted not only by the mentor to the mentee but also carried out in groups of mentee by exchanging experiences and discussions to find solutions for constraints/problems by themselves when implementing ACTIVE activities. Mentoring activities are expected to keep up the morale of the cadres as dengue control agents in the field, but will also become a means of strengthening the cadres' commitment to remain an active agent of health within their neighborhood after activities of the ACTIVE program end.
Results of the ACTIVE program can be seen from the Free of Larva Rate (ABJ), or Container Index (CI), which shows numbers before and after the ACTIVE program, became effective in the community. ABJ or CI is obtained from HIS and HEWS development and is derived from cadres reporting PJR and PSN. The reporting application SMS Gateway has not been conducted in all Community Units in each Administrative Village. However, the chart data is able to represent quantitatively the results of the ACTIVE program in the six pilot project regions.
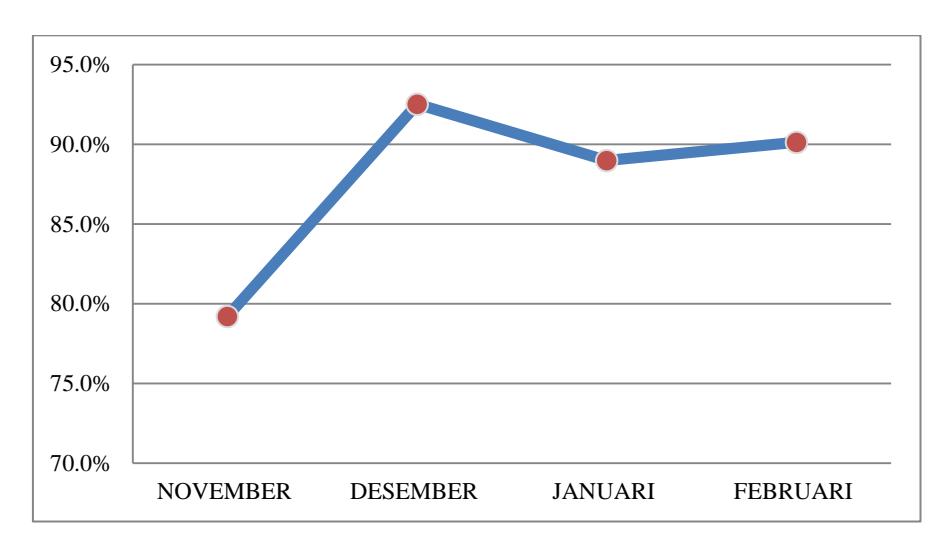
Figure 3. Free of Larva Rate (ABJ) in the school environment of the ACTIVE pilot projects November 2015- February 2016 Source: ACTIVE Team, 2016
Figure 3 illustrates an ABJ graph in school surroundings during the last four months of implementation of ACTIVE activities. There was a decrease in the ABJ rate from 92.5% in December to 89% in January. In addition to the increased intensity of rainfall, the school holiday schedule in early January decreases the intensity of PJR and PSN by small doctors. This increases the potential for greater development of mosquito breeding sites due to decreased dengue control efforts. However, the increased PSN activity after the end of school holidays has raised ABJ to 90.1% in February.
Figure 4 shows an upward trend of ABJ in the six pilot project regions. In the early implementation of the program in September, this amounted to 89.2%, fluctuating up to 92% in February. A positive result is indicated in the initial five months of the implementation of the ACTIVE program in the community. However, when the rain intensity increased after January, ABJ declined. Something else that indicates good results are changes in clean and healthy behavior that are started to be felt in the communities and schools. This relates to the efforts of cadres in campaigning for a Clean and Healthy Lifestyle (PHBS) during house visits.
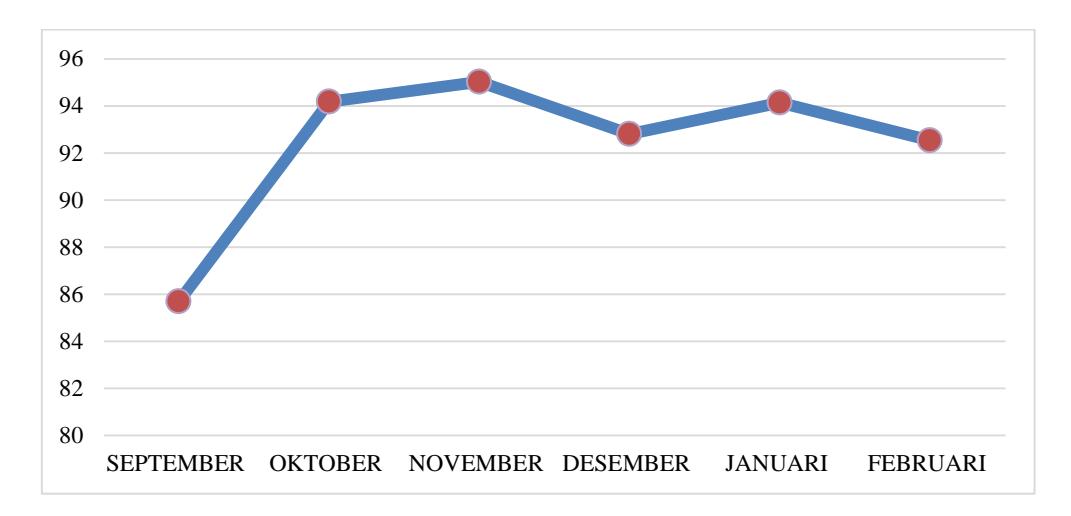
Figure 4. Free of Larva Rate (ABJ) in the ACTIVE pilot project communities in September 2015- February 2016 Source: ACTIVE Team, 2016
Empowerment of cadres of larva monitoring (jumantik) in dengue mosquito breeding site eradication (PSN) has a significant influence on the increase in Free of Larva Rate (ABJ). The form of community participation that is most effective in the control of dengue is to empower larva-monitoring cadres (Chadijah et al, 2011). In contrast to the implementation of activities in schools that are bound by the schedule of teaching and learning activities, dengue control activities in the community are more intensively conducted by the cadres. The role of cadres is very important as health agent able to involve the community so dengue control can be more effective.
The community hopes that this activity will not end with the completion of the series of ACTIVE activities. The government is expected to facilitate a dengue control program that is similar or even better innovated. Madam Indarsih, as facilitator, gives her testimony,
"The ACTIVE Program changes people's behavior to become more sensitive to the cleanliness of the home environment, especially regarding mosquito breeding sites. ABJ in my neighborhood rose by 90%. I hope that the government can continue with a program similar to ACTIVE next year"
Alternative Approaches
The term alternative approach emerged as a response and attempt to supplement and strengthen the efforts of various dengue prevention programs of the government. One example of government efforts is the fogging program, which uses chemical fumigation against mosquito breeding sites in the surroundings of houses. Implementation of this program has not been able to touch upon the principal problems in society, namely the need to change behavior to be clean and healthy. An alternative approach based on participation is one of the alternative methods used in the ACTIVE Program and focuses more on increased involvement of stakeholders in each activity.
Alternative approaches can be regarded as collaborative social learning and inclusive planning. Social learning theory developed by Albert Bandura considers that direct observation and experience is a form of model that is used by everyone to learn. Individuals will learn to imitate the behavior of others who become their model (Bandura, 1977). Niewolny & Wilson in their research revealed that social learning has been recognized as an important perspective in understanding problems in a social context, in particular, the scope of adults. Social learning can be understood as a means of regulating and developing adult education, which can be seen from factors of behavior, cognitive aspects, and constructive psychology (Merriam, 2011). In the ACTIVE program, the successful transfer of skills and knowledge to the cadres or the public is an application of the method of adult learning, which became one of the alternative approaches. From the perspective of the ACTIVE Project, adult learning is capacity building of knowledge and skills with the approach of an adult way of thinking. The community as a target as well as participant is considered adult and fit to receive material through such methods. Adjustment of the condition of society and the methods used is instrumental in the success of this program.
On the other side, success in involving various government levels with the community is an application of inclusive planning which is a basic premise of this ACTIVE program. Inclusive planning is motivated by the concept of urban planning that touches upon all aspects of community life, one of which is the health aspect. The stakeholders should work together to integrate their need for a healthy urban environment (Malhotra, 2010). The government must be able to facilitate actions and policies that can strengthen public participation in policy-making in the health sector, including in terms of funding, education, training/education, up to involvement in decision-making (Frankish et al, 2002; Hancock, 1999). The existence of the ACTIVE program can bridge the relationship and coordination between the government and the public that has been valued not optimal, particularly in the field of health control of dengue.
The involvement of all stakeholders with interests in dengue outbreaks in Semarang is a form of inclusive planning initiated with advocacy techniques done by MCI towards the government (Health Department) and policy makers at the level below it. On the other hand, the ACTIVE Program carries out a participatory approach by inviting the public to play a more active role, either as facilitators for other residents or by becoming a cadre in their environment.
Conclusion
The ACTIVE program that was carried out in the city of Semarang uses different approaches from dengue outbreak control programs in general. An alternative approach based on the concept of social learning and inclusive planning is able to get the government's attention and arouse the enthusiasm and the spirit of community in facing dengue in their region. Based on interviews with stakeholders, they generally refer to the alternative approach based on participation as interesting and consider the approaches effective in solving the problems of dengue at the level of public behavior. Although it is not an easy task and requires a long process, changing of people's behavior is a strategy should be the basis of dengue control efforts (Willis and Atkinson, 2005). The ACTIVE program is expected to establish a culture of a clean and healthy lifestyle for the long term, not only to prevent dengue disease but also potential other diseases in the community's environment.
The model of community capacity building in facing dengue as carried about by Suwanbamrung et al (2011) and the strategy of community development of Carmen et al (2005) can be combined with the alternative approaches of the ACTIVE program, with adjustment of phases. The implementation of the ACTIVE program was effective in the community, which is evident from the significant increase in Free of Larva Rate (ABJ). However, there is still a fluctuation in the application in the school environment. This requires an evaluation of the implementation of ACTIVE activities. Nevertheless, changes occur in community behavior and the school
community pays attention to cleanliness of their environment, especially to potentially mosquito breeding sites.
Figure 4 shows an upward trend in Free of Larva Rate (ABJ) in the six pilot project regions at the start of program implementation. ABJ increased from 89.2% in September 2015 to 95% in January 2016. This shows the positive results for the five months after the direct intervention by the ACTIVE program in the community. Something else that showed good results are changes in clean and healthy behavior that start to be felt in the communities and at schools. This relates to the efforts of cadres in the campaign for healthy and clean behavior during house visits.
The challenges ahead lie in the efforts to maintain the continuity, which the government should ensure together with the community so activities and systems that have been established in the ACTIVE program can continue to be performed. An alternative approach based on participation is expected to be a capital that governments and communities can use to transfer skills and knowledge to prospective facilitators, cadres, and society in a broader scope after the ACTIVE program is completed.
Acknowledgment
The research, writing and/or publication of this article received financial support from the Rockefeller Foundation through Mercy Corps Indonesia which works together with government agencies in Semarang (the Regional Development Planning Agency (BAPPEDA), the Health Department, the Department of Education, the Meteorology Climatology and Geophysics Agency (BMKG), NGOs, IUCCE (Initiative for Urban Climate Change and Environment) and academics from the Department of Urban and Regional Planning, University of Diponegoro.