
Introduction
The COVID-19 pandemic has disproportionately affected vulnerable populations, including persons with disabilities (PWDs), indigenous peoples (IPs), women, children, senior citizens, and immunocompromised individuals (Sarmiento et al., 2020; Akter et al., 2018). These groups face higher health risks and more barriers in accessing healthcare services, making it critical for healthcare facilities to address their unique needs.
Representatives from vulnerable groups requested health services to provide virtual sign language interpretation services during the pandemic, rooted in the mandates of Philippine Republic Act 11106 and Batas Pambansa 344. Civil society organizations appealed for active observance of gender and development policies and the establishment of helpdesks for gender-based violence against women and children services. They called for implementing the Philippine Indigenous People's Rights Act of 1997 and related guidelines to provide accessible health services for indigenous peoples. In response, the Philippines COVID-19 Emergency Response Project (PCERP), funded by the World Bank, initiated interventions to raise awareness of vulnerable groups' needs during health emergencies like COVID-19. PCERP formulated policies to develop a self-assessment tool for HCFs and an action plan to improve the accessibility of services for vulnerable groups. This study consolidated the responses of participating HCFs to the selfassessment survey conducted in December 2021, as they reviewed their compliance with the standards and guidelines on catering to the needs of PWDs, IPs and indigenous cultural communities (ICCs), women and children, senior citizens, as well as immunocompromised individuals.
Despite the urgent need to ensure that vulnerable groups have access to essential healthcare services during a pandemic, limited research has been done on the capacity of healthcare facilities (HCFs) in the Philippines to accommodate the needs of these populations. Existing studies have highlighted the challenges faced by vulnerable groups in accessing healthcare services (Bhatt & Bathija, 2018; Gudlavalleti, 2018), but there is a lack of comprehensive assessments of HCF's readiness to serve these groups, particularly in the context of the COVID-19 pandemic. In this study, therefore, we aimed to determine the capacity of HCFs in the Philippines to provide accessible and quality health services to vulnerable groups during the COVID-19 pandemic. Specifically, we sought to:
- 1. Assess the physical infrastructure, equipment, personnel capacity, and health promotion materials of HCFs in relation to serving vulnerable populations.
- 2. Identify gaps and areas for improvement in HCFs' capacity to serve vulnerable groups.
- 3. Provide recommendations for targeted interventions, policies, and resource allocation to enhance healthcare accessibility for vulnerable populations.
Our study contributes to the limited body of knowledge on healthcare accessibility for vulnerable groups in the Philippines, particularly during health emergencies like the COVID-19 pandemic. We deliver insight into the predisposing, enabling, and need factors influencing healthcare utilization among these populations by applying the Andersen behavioral model (ABM) as a theoretical lens. Our findings can inform the development of targeted interventions and policies to improve HCFs' capacity to serve vulnerable groups and promote health equity in the country.
Literature review
In this section, we review the existing literature on vulnerable populations, healthcare facilities, and the Andersen behavioral model to give context to our study on the accessibility of healthcare services for vulnerable groups in the Philippines during the COVID-19 pandemic.
Vulnerable populations
In this study, we defined vulnerable populations as groups disproportionately affected by health risks and facing significant barriers to accessing healthcare services due to social, economic, and cultural factors (Arnaut et al., 2021). These groups include persons with disabilities (PWDs), indigenous peoples (IPs), women, children, seniors, and immunocompromised individuals, among others (Sarmiento et al., 2020; Akter et al., 2018). Vulnerable populations often experience marginalization, discrimination, and lack of access to resources, which can exacerbate their health vulnerabilities, particularly during health emergencies like the COVID-19 pandemic (Gabrani et al., 2021; Ogunlade & Ogunfowokan, 2021).
Previous studies have highlighted the specific challenges these groups face in accessing healthcare services. PWDs, for example, may face physical barriers to accessing healthcare facilities, as well as communication barriers and discrimination from healthcare providers (Kuper et al., 2021; Gudlavalleti, 2018). Indigenous peoples often experience cultural and linguistic barriers, as well as geographic isolation, which can limit their access to healthcare services (Barnett et al., 2021; Crowshoe et al., 2021). Women and children, particularly those from lowincome households, may face financial barriers and lack of transportation, preventing them from seeking necessary healthcare (Bhatt & Bathija, 2018; Sharma et al., 2021).
To address these inequalities, we have found researchers emphasizing the importance of community-based interventions, such as mobile health clinics and telemedicine services (Kuper et al., 2021; Bhatt & Bathija, 2018), as well as the role of community health workers in bridging the gap between vulnerable populations and healthcare systems (Carter et al., 2021; Hartzler et al., 2018). However, there is a lack of comprehensive research on the barriers to healthcare access for vulnerable groups in the Philippines, particularly during the COVID-19 pandemic.
Healthcare facilities
We defined healthcare facilities in this study as institutions that provide healthcare services, including hospitals, clinics, health centers, and rural health units (DOH et al., 2013). Healthcare facilities are crucial in providing accessible and quality healthcare services to vulnerable populations. However, many healthcare facilities in low- and middle-income countries, including the Philippines, face challenges in terms of physical infrastructure, equipment, personnel capacity, and health promotion materials tailored to the needs of vulnerable groups (Oberoi et al., 2016; Martinez et al., 2020).
Studies in the Philippines have shown that community-based health programs and mobile health technologies can improve healthcare utilization among vulnerable populations (Collado, 2019; Toquero, 2021). The role of community health workers has also been highlighted in bridging the gap between indigenous communities and healthcare providers (Barnett et al., 2021; Iseghem et al., 2023). Healthcare financing programs, such as the Philippine Health Insurance Corporation (PhilHealth), have been found to increase healthcare utilization among poor households (Venkataramanan et al., 2022).
However, despite these efforts, healthcare facilities in the Philippines still face challenges in providing accessible and inclusive services to vulnerable groups, particularly during health emergencies like the COVID-19 pandemic (Velasco et al., 2021; Valdez et al., 2021). It also shows limited research on the capacity of Philippine HCFs to provide accessible services to these groups.
The Andersen behavioral model of healthcare use
The Andersen behavioral model (ABM), as illustrated in Figure 1, has been a game-changer in understanding what drives people to seek healthcare services. It is like a roadmap that helps to navigate the complex world of healthcare utilization. At its core, the ABM tells us that there are three main factors that influence whether someone will actually go to the doctor or not: predisposing factors, enabling factors, and need factors (Andersen, 1995). Predisposing factors are all about the individual – their age, gender, ethnicity, and even their beliefs about health. It is the stuff that makes us who we are and shapes our attitudes toward healthcare. Enabling factors, on the other hand, are practical things that make it easier or harder for us to access care, like how much money we have, whether we have health insurance, and if we can even get to the doctor's office. Finally, need factors are about how we perceive our own health and how sick we actually are (Andersen, 1995).
When it comes to vulnerable populations, the ABM is particularly useful in helping to understand the unique challenges they face in accessing healthcare (Li et al., 2017). For example, cultural beliefs and social stigma can be major predisposing factors that prevent people with disabilities or indigenous populations from seeking care (Gudlavalleti, 2018; Crowshoe et al., 2021). Similarly, lack of transportation and financial constraints can be significant enabling factors that limit healthcare access for low-income women and children (Bhatt & Bathija, 2018; Sharma et al., 2021).
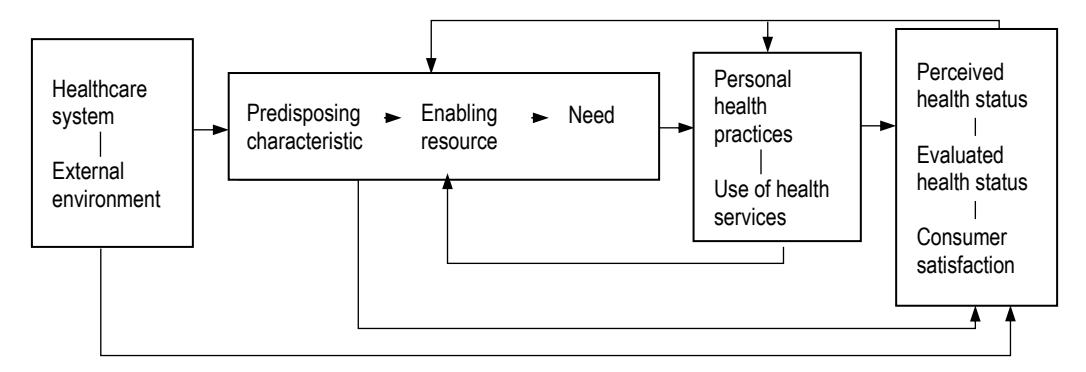
Figure 1. Andersen's behavioral model of healthcare use. (Source: Authors' adaptation of Andersen's model as a theoretical lens for this research on improving healthcare facility services for vulnerable populations)
In our study, we used the ABM as a lens to analyze the results of a self-assessment survey of healthcare facilities in the Philippines during the COVID-19 pandemic. We could identify the specific predisposing, enabling, and need factors that contribute to healthcare inequalities and their impact on health facilities in the country by looking at the data through the ABM framework (Li et al., 2017). It is like putting together a puzzle – each piece of information helps to build a more comprehensive picture of what is happening. The behavioral model is a powerful tool that helps to understand the complex factors influencing healthcare utilization, especially among vulnerable populations. We hoped to shed light on the challenges and opportunities for improving healthcare accessibility in the Philippines and beyond by using this lens in our study.
Research inspiration and gaps
The existing literature on vulnerable populations, healthcare facilities, and the Andersen behavioral model gave us insight into the predicaments of healthcare accessibility. These are, however, notable research gaps and limitations in the current body of knowledge. Firstly, there is a lack of comprehensive assessments of HCFs' capacity to serve vulnerable groups in the Philippines, particularly during health emergencies like the COVID-19 pandemic. Secondly, the specific barriers and facilitators to healthcare access for vulnerable populations in the Philippine context remain underexplored. Thirdly, the application of the ABM to guide the analysis of healthcare accessibility for vulnerable groups in the Philippines is also limited.
We want to help address these research gaps by conducting a comprehensive assessment of HCFs' capacity to serve vulnerable populations in the Philippines during the COVID-19 pandemic. Based on Andersen's theoretical framework, we wish to present a more sophisticated understanding of the factors influencing healthcare utilization among these groups. Our findings may inform the development of targeted interventions, policies, and resource allocation strategies to improve healthcare accessibility for vulnerable populations in the Philippines. Moreover, our study has the potential to contribute to the broader body of knowledge on healthcare accessibility and equity, with implications for policy, practice, and future research.
Materials and methods
Operational framework
In this study, we set out to understand the factors that influence healthcare accessibility for vulnerable groups in the Philippines and to identify the challenges these groups face when seeking care. To guide our research, we turned to Andersen's (1995) behavioral model, which has proven to be a valuable tool for examining the complex interplay of factors that shape healthcare utilization. At the heart of the model are three key components: predisposing factors, enabling factors, and need factors. Predisposing factors include demographic characteristics, social structure, and health benefits – all of which can influence an individual's likelihood to seek care. Enabling factors, such as the availability and accessibility of healthcare services, financial resources, and health insurance coverage, can either facilitate or hinder access to care. Finally, need factors, encompassing perceived and actual health needs, drive the decision to seek healthcare services.
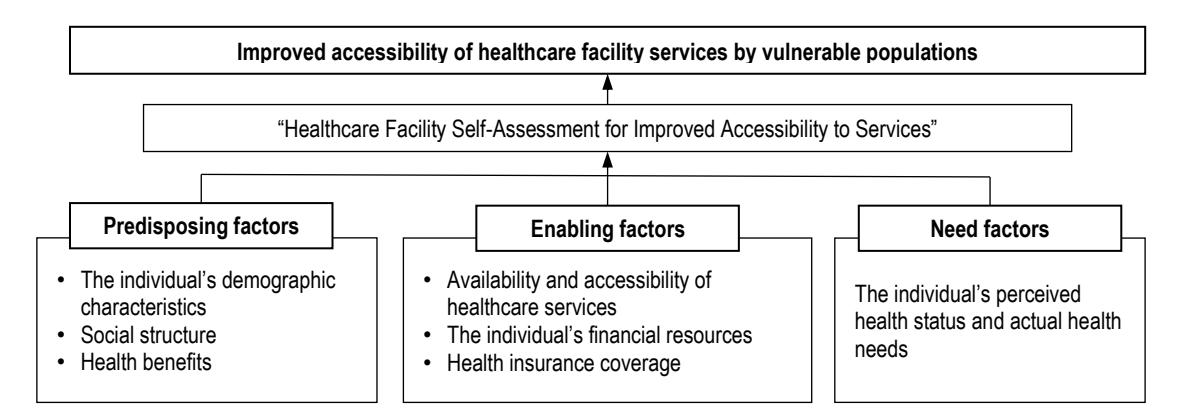
Figure 2. Conceptual framework for improved healthcare facilities for vulnerable populations. (Source: Authors' illustration as inspired by Andersen's behavioral model)
Although the ABM delivers a solid foundation for understanding healthcare accessibility, we recognize that vulnerable groups face unique challenges that need to be addressed. These challenges include physical barriers, such as inaccessible healthcare facilities; financial barriers, such as the inability to afford healthcare services; cultural and linguistic barriers that can hinder
effective communication with healthcare providers; and stigma and discrimination, which can discourage individuals from seeking care altogether. To gain a comprehensive understanding of these challenges and to assess the capacity of healthcare facilities to provide accessible services to vulnerable groups, we used the Healthcare Facility Capacity Self-Assessment Survey (see Table 1). The survey helped us to identify gaps and deficiencies in the current healthcare system that may be preventing vulnerable groups from accessing the care they need by evaluating these components.
Conducting this study was not without its challenges, but we were motivated by the potential impact of our findings. Through the assessment, we present evidence-based recommendations for improving the capacity of healthcare facilities to serve these populations. We designed our operational framework, as illustrated in Figure 2, to serve as a roadmap for understanding and addressing the complex factors that influence healthcare accessibility. We strove to create a study, guided by this operational framework, that could make a meaningful difference in the lives of those who need it most by combining the ABM with a comprehensive self-assessment survey and a deep understanding of the unique challenges these groups face.
Research design
We applied a cross-sectional descriptive quantitative research design to assess the capacity of healthcare facilities in providing accessible services to vulnerable populations in the Philippines (Creswell, 2021). This design allowed us to collect data simultaneously from a sample of healthcare facilities and describe their characteristics and capacity to serve vulnerable groups (Setia, 2016). Our study's operational framework, based on Andersen's (1995), relates to the development of the Healthcare Facility Capacity Self-Assessment on the Accessibility of Services for Vulnerable Populations Survey.
The self-assessment tool, as shown in Table 1, was developed based on various DOH (and DPWH) policies, standards, and guidelines related to servicing vulnerable groups (DOH et al., 2013; DOH, 2015). It covers four main components: physical infrastructure, equipment, personnel capacity, and health promotion materials. The physical infrastructure components assess the accessibility of healthcare facilities' built environment, including ramps, handrails, corridors, walkways, toilets, and signage (DOH et al., 2013; DOH, 2015). The equipment component evaluates the availability of assistive, emergency, communication, and culturesensitive equipment (DOH et al., 2013; DOH, 2015). The personnel capacity component assesses the knowledge, skills, and training of healthcare personnel in serving vulnerable populations, including PWDs, IPs, women, children, and seniors (DOH et al., 2013; DOH, 2015). The health promotion materials component evaluates the availability and accessibility of information, education, and communication (IEC) materials tailored to the needs of vulnerable populations (DOH et al., 2013; DOH, 2015). In addition to these, the inclusivity checklist for health promotion playbooks, with eight indicators, was also incorporated to determine the feedback on the respective information and education campaigns from HCFs (DOH et al., 2013; DOH, 2015).
The self-assessment tool consisted of 62 original indicators across these four components. It used a checklist format with 31 physical infrastructures, 7 equipment, 15 personnel, and 9 health promotion indicators. However, another 8 were added under the health promotion playbook inclusivity indicators, each with binary yes/no responses to indicate compliance. The tool was reviewed and validated by technical experts from various DOH offices to ensure its relevance and appropriateness (Boateng et al., 2018).
According to the Department of Health, there were 1,244 licensed hospitals and 2,592 government-owned primary care facilities in the Philippines as of December 2020 (DOH et al., 2013; DOH, 2015). Given the country's large number of healthcare facilities, we used purposive sampling to select 154 facilities across different regions, ownership types, and service capacities. This included private hospitals (n = 68, 44%), local government hospitals (n = 61, 40%), DOH hospitals (n = 24, 16%), and other facilities like infirmaries and rural health units (Flores et al., 2021). Participating facilities ranged in service capacity from level I to level III. Adequate regional representation and heterogeneity of healthcare facility type and capacity allowed for greater generalizability of the results. While the sample size may not be representative of all healthcare facilities in the Philippines, it still displays a diverse range of perspectives and experiences that can inform our understanding of the challenges and opportunities in providing accessible services to vulnerable populations (Palinkas et al., 2015).
We administered the self-assessment survey online using Google Forms and distributed it to the sampled healthcare facilities from December 2021 to January 2022. Facility administrators or their designated representatives completed the survey. Quantitative descriptive statistical analysis was conducted using Excel software. Frequency counts and percentages were calculated for each survey indicator to determine the proportion of participating healthcare facilities meeting the criteria. This analysis identified strengths, deficiencies, and gaps across the original four selfassessment components to reveal insights into facilities' capacity to serve vulnerable populations (Sullivan & Artino, 2013).
Table 1. HCF self-assessment for improved accessibility to services.
Component Indicator
Physical infrastructure (DOH et al., 2013; DOH, 2015)
- PI1 Entry ramp(s) is/are provided when access to the health facility's entrance is not on the same level as the ground, with a minimum clear width of 1.22 meters (or 4 feet) in one direction (or 2.44 m or 8 ft in two opposite directions), slope not steeper than 1:12 m, 1.5-m ramp landing for ramp slope with 1:12 gradient, and handrails at both sides. The maximum ramp length is 6 m, and the ramp's top and bottom level area should be 1.8 m.
- PI2 Handrails are provided at the ramp's sides, 1.8 m from the ramp's foot, for ramps with a rise greater than 0.20 m. The handrails' height should be 0.7 m to 0.9 m and 1.0 m to 1.06 m handrail location at great heights. The handrails should be 30 mm to 50 mm in diameter, and the handrail extension at 300 mm.
- PI3 Access corridors for patients using beds or stretchers and equipment are available and at least 2.44 m (or 8 ft) in clear width, which can accommodate two-wheeled stretchers alongside each other, and 1.83 m (6 ft) for corridors not commonly used.
- PI4 Walkways are provided with adequate passageways, with a minimum of 1.2 m width and a 1:20 or 5 percent preferred gradient.
- PI5 A multi-level ramp or elevator is provided for ancillary, clinical, and nursing areas not located on the health facility's upper floor, free from obstruction for patients with special needs, with a slope not steeper than 1:12 m.
- PI6 A functional elevator capable of accommodating at least one patient bed is provided in case there is no multi-level ramp strategically placed for PWDs (i.e., near the facility's service areas), with non-slip materials, braille-sign buttons/controls at a height reachable by the seated individual, and audio announcement system. Signages should be placed to inform PWDs of the elevator/slide ramp's location.
- PI7 A minimum of one (1) parking space for every twenty-five (25) beds, with sufficient space for PWDs, is provided to allow easy transfer from the car park to ingress/egress levels, located in the area nearest building entrances with provision for bicycle parking.
- PI8 The main door, including the common service areas, has a minimum clear opening of 0.90 m, with a maximum of 1.20 m, to easily accommodate patients regardless of movement type.
- PI9 Doors used for emergency exits must always lead directly outside the building to an open area, such as a court, yard, street or alley, interior and exterior stairs, and ramp, with proper signage and directions present.
- PI10 Water closets have a minimum area of 1.70 x 1.80 m, with a turning space of 2.25 m2 , and a minimum dimension of 1.50 m for wheelchairs in water closet stalls/cubicles for enabling lateral mounting.
- PI11 In water closets, one movable grab bar and one fixed grab bar to the adjacent wall are installed in the stall/cubicle for lateral mounting. Fixed grab bars on both sides of the wall shall be installed for stalls/cubicles for frontal mounting.
- PI12 A ratio of one toilet for every eight patients or personnel is observed for hospitals. There are toilets with handwashing stations in the following areas: administrative service area or lobby, dietary, emergency room, out-patient department, surgical and obstetric service, labor room, patient room, isolation room, clinical laboratory, and X-ray room.
- PI13 Separate water closets/toilets for staff, patients, and visitors are available.
- PI14 Separate water closets/toilets for male, female, and LGBTQIA+ (if applicable) patients and personnel are available.
- PI15 For hospitals, a minimum of one water closet/toilet on each floor is provided that is accessible to PWDs and patients with decreased mobility.
- PI16 Water closets/toilets have bin(s) for waste disposal generated from menstrual hygiene and a wash area with a constant water supply.
- PI17 Water closets/toilets have diaper-changing areas.
- PI18 Hygiene closets/toilets have available or nearby facilities or vending machines with hygiene commodities (e.g., sanitary napkins).
- PI19 Floors are made of non-skid/slip material, easy to clean, and resistant to chipping.
- PI20 Seating for PWDs is accessible from the main lobby to primary entrances and related toilet facilities.
- PI21 Positional, directional, and warning tactile blocks are available for blind patients, visitors, or personnel.
- PI22 A private room or space with visual and acoustic privacy is available and dedicated to handling cases and clients with concerns about gender-based violence, violence against women and children, and HIV/AIDS.
- PI23 Lactation or breastfeeding area(s) are available for patients, outpatients, clients, and hospital staff.
- PI24 A culture-sensitive unit or area is available and dedicated to indigenous peoples/indigenous cultural communities-related concerns and for indigenous peoples' systems and practices on health, such as rituals made of bamboo and not concrete (if applicable) especially for health facilities catering IPs/ICCs based on geographical location.
- PI25 A perimeter fence around the healthcare facility is present, especially in geographically isolated and disadvantaged areas (GIDAs).
- PI26 Provision of hygiene materials, such as disinfectants (alcohol/sanitizer), handwashing facility, and/or foot bath at the healthcare facility entrance/exit.
- PI27 Provision of the temperature-scanning device at the facility entrance/exit.
- PI28 Directional signages are prominently posted to help locate service areas within the organization and placed on walls and doors at a minimum of 1.40 m to a maximum of 1.60 m height.
- PI29 Contents and specifications of signages are consistent with the standard specifications set forth by the DOH's Signage and Systems Manual for Hospitals and Offices (1994).
- PI30 Express lanes for vulnerable groups (e.g., senior citizens, IPs/ICCs, and PWDs) and violence/harassment-related cases.
- PI31 Waiting area for patients and visitors, especially for vulnerable groups and violence/harassmentrelated cases in the hospital lobby, emergency room, and outpatient department, among others.
Equipment (DOH et al., 2013; DOH, 2015)
- E1 The facility has available ambulatory care devices for emergency cases, especially for vulnerable groups and violence-related cases.
- E2 The facility has audio and visual alarm systems for emergencies.
- E3 The facility has functional and dedicated hotlines for COVID-19 and violence-related concerns.
- E4 The facility has a dedicated device that can be repurposed for telemedicine and virtual sign language interpretation services for PWDs in various service areas, such as in the emergency rooms, doctors' clinics, and COVID-19-related service areas, such as wards/rooms, testing center, and isolation areas/tents.
- E5 The facility has stable signal and/or internet access, preferably 100 Mbps, which will enable telemedicine or virtual sign language interpretation services for PWDs in various service areas, such as in the emergency rooms, doctors' clinics and COVID-19-related service areas, such as wards/rooms, testing center, and isolation areas/tents.
- E6 A database of healthcare workers and clients who access telemedicine facilities and services disaggregated by sex, presence of disability, and affiliation with an IP/ICC is available.
- E7 The facility has available culture-sensitive equipment, such as beds made of bamboo (if applicable), especially for health facilities catering to IPs/ICCs based on geographical location.
Personnel capacity (DOH et al., 2013; DOH, 2015)
- PC1 The facility has staff knowledgeable and trained in operating telemedicine devices.
- PC2 The facility has staff knowledgeable and trained on disability sensitivity and sign language interpretation for PWDs, with experience in healthcare settings and fluency in medical terms, especially on COVID-19.
- PC3 Personnel receives regular/continuous training on Filipino sign language (FSL) interpretation, especially with medical orientation.
- PC4 A referral pathway and helpdesk for PWDs are in place to connect the patients with experts in case the facility has no in-house trained personnel.
- PC5 The facility has staff knowledgeable and trained on gender-responsive health service delivery (e.g., training on basic gender and development orientation, gender-sensitivity, service-specific training with gender-sensitivity dimensions, and code of conduct).
- PC6 The facility has a women and children protection unit (WCPU) with staff knowledgeable and trained on handling gender-based violence and violence against women and their children-related cases.
- PC7 A referral pathway is in place to connect the patients with experts on cases related to GBV and VAWC in case the facility has no WCPU or in-house trained personnel.
- PC8 Personnel receives regular and continuous GAD, GBV, and VAWC training.
- PC9 The facility has staff knowledgeable and trained in providing services to IPs/ICCs, with a background in cultural sensitivities and traditional medicine, and has undergone culture-sensitivity training (if applicable), especially for health facilities catering IPs/ICCs based on geographic location.
- PC10 A dedicated unit in the facility is present for IP/ICC-related concerns and a referral pathway for connecting patients with experts on IP/ICC concerns (if applicable), especially for health facilities catering to IPs/ICCs based on geographic location.
- PC11 Personnel receives regular/continuous training on culture sensitivity (if applicable), especially for health facilities catering IPs/ICCs based on geographic location.
- PC12 Personnel receives training on empathetic communication and risk communication and community engagement (RCCE) using the DOH-HPB and UNICEF module on RCCE for healthcare workers during and after the pandemic.
- PC13 The facility has dedicated staff (e.g., health education and promotion officer) knowledgeable and trained in health promotion, health or science communication, and education receives regular training.
- PC14 The facility has a dedicated staff who coordinates with the local health office's health promotion unit for the counterpart prevention-side initiatives to eliminate violence against women, young boys and girls, elderly, IPs/ICCs, and the LGBTQIA+ who are at risk of abuse and violence.
- PC15 The facility has a dedicated mental and psychological support unit with staff receiving continuous training.
Health promotion materials (DOH et al., 2013; DOH, 2015)
- HP1 The facility has printed visual promotion materials on COVID-19 posted in conspicuous areas. The staff can answer basic COVID-19 questions/concerns.
- HP2 The facility has recorded audio promotion materials on COVID-19 played in conspicuous areas through a public address (PA) system or megaphone. The staff can answer basic COVID-19 questions/concerns.
- HP3 The facility has printed visual instructional materials on COVID-19 testing posted in the testing center/service area and conspicuous places. The staff can answer basic COVID-19 questions/concerns.
- HP4 The facility has printed visual promotion materials on hand hygiene and sanitation or other COVID-19 prevention measures (e.g., BIDA campaign) posted in conspicuous areas. The staff can answer basic questions/concerns on hand hygiene and sanitation.
- HP5 The facility has recorded audio promotion materials on COVID-19 prevention measures (e.g., BIDA campaign videos) played in conspicuous places through a PA system or megaphone. The staff can answer basic questions/concerns on hand hygiene and sanitation.
- HP6 The facility has printed signages/information materials on services for PWDs posted in conspicuous places and information on the dedicated unit handling PWD-related concerns.
- HP7 The facility has printed signages/information materials on services for gender-related concerns, sexual harassment, and VAWC posted in conspicuous places and information on the dedicated WCPU or helpdesk.
- HP8 The facility has printed signages/information on sexual and reproductive health services.
- HP9 The facility has printed signages/information materials translated in accordance with the ethnicity of the dominant IP/ICC communities in the area, including service information for IPs/ICCs posted in conspicuous areas and information on the dedicated unit handling those concerns (if applicable), especially for health facilities catering IPs/ICCs based on geographic location.
Health promotion playbooks (DOH et al., 2013; DOH, 2015)
- HPB1 Are members of the vulnerable groups, their respective organizations or associations, and government and non-government organizations included in planning the proposed intervention/program?
- HPB2 Is the program non-discriminating, wherein it guarantees that human rights are exercised without discrimination of any kind based on race, color, sex, language, religion, politics, property, birth, or other statuses, such as disability, age, marital and family status, sexual orientation and gender identity, health status, residence, and economic and social situation?
- HPB3 Are IEC materials placed in conspicuous areas to provide a clear line of sight to any seated or standing user?
- HPB4 Are all beneficiaries safe, private, and security protocols in place?
- HPB5 As needed, are accessible communication materials available for vulnerable groups (e.g., sign language interpreter for video materials, text-to-speech for print materials, captioning, etc.)?
- HPB6 As needed, are capacity-building modules, communication materials, and FAQs available in the pilot community's local dialect?
- HPB7 Is the health promotion intervention free from any physical barrier that could prevent someone from fully maximizing the intervention?
- HPB8 Is the health promotion intervention free from any procedural barrier that could prevent someone from fully maximizing the intervention?
Source: Authors' adoption of the assessment instrument (DOH et al., 2013; DOH, 2015).
Results
Descriptive statistics
To implement this self-assessment survey, all healthcare facilities, regardless of ownership and service capacity, were encouraged to participate by issuing Department Circular 2021-0545. Table 2 shows 154 HCFs submitted their input to this initiative, with the National Capital Region (NCR) having the highest number of submissions with 70 facilities. The breakdown of respondents in other major categories was as follows: HCFs from eleven regions submitted their responses for the self-assessment survey. Regarding ownership type, Table 2 also shows that most respondents came from private hospitals (68, 44%), followed by local government hospitals/facilities (61, 40%). There were 24 (16%) participants from DOH hospitals/facilities, and the PNP General Hospital (1%) also participated as another government HCF.
Table 2. Breakdown of respondents into regions and ownership type.
| Region | DOH hospital | LGU facility | Private hospital | Other government HCF | Total |
|---|---|---|---|---|---|
| CAR | 1% (1) | 3% (5) | 1% (1) | 0 | 5% (7) |
| CARAGA | 0 | 3% (5) | 1% (1) | 0 | 4% (6) |
| NCR | 6% (10) | 6% (9) | 33% (51) | 0 | 45% (70) |
| Region I | 0 | 1% (2) | 0 | 0 | 1% (2) |
| Region II | 1% (2) | 2% (3) | 1% (1) | 0 | 4% (6) |
| Region III | 1% (1) | 2% (3) | 1% (1) | 0 | 3% (5) |
| Region V | 0 | 2% (3) | 0 | 0 | 2% (3) |
| Region VI | 0 | 1% (1) | 0 | 0 | 1% (1) |
| Region VIII | 1% (2) | 0 | 1% (2) | 0 | 3% (4) |
| Region X | 5% (8) | 12% (9) | 6% (9) | 0 | 23% (36) |
| Region XI | 0 | 7% (11) | 1% (2) | 1% (1) | 9% (14) |
| Total | 16% (24) | 40% (61) | 44% (68) | 1% (1) | 100% (154) |
Source: Author's compilation based on statistical results
There was representation in almost all service capacity categories per region. Submissions, as we present in Table 3, came from levels I, II, and III HCFs, infirmaries, health centers, quarantine facilities, and one treatment and rehabilitation center. Most respondents came from level I HCFs (50, 33%), followed by level III (35, 23%), infirmaries (28, 18%), health centers (18, 12%), quarantine facilities (3, 2%), and level II and treatment and rehabilitation centers (1, 1%). However, there were more level-III HCFs that participated in the NCR.
| Region | Level I | Level II | Level III | Infirmary TRC | Quarantine facility | Health center | Total | |
|---|---|---|---|---|---|---|---|---|
| CAR | 1% (1) | 0 | 1% (2) | 2% (3) | 0 | 0 | 1% (1) | 5% (7) |
| CARAGA | 2% (3) | 0 | 0 | 1% (2) | 0 | 0 | 1% (1) | 4% (6) |
| NCR | 6% (10) | 1% (1) | 19% (29) | 2% (3) | 0 | 2% (3) | 2% (3) | 45% (70) |
| Region I | 1% (2) | 0 | 0 | 0 | 0 | 0 | 0 | 1% (2) |
| Region II | 3% (4) | 0 | 0 | 1% (1) | 0 | 0 | 1% (1) | 4% (6) |
| Region III | 1% (1) | 0 | 1% (1) | 2% (3) | 0 | 0 | 0 | 3% (5) |
| Region V | 1% (1) | 0 | 0 | 1% (2) | 0 | 0 | 0 | 2% (3) |
| Region VI | 0 | 0 | 0 | 0 | 1% (1) | 0 | 0 | 1% (1) |
| Region VIII | 1% (1) | 0 | 1% (2) | 1% (1) | 0 | 0 | 0 | 3% (4) |
| Region X | 16% (24) | 0 | 1% (1) | 4% (6) | 0 | 0 | 3% (5) | 23% (36) |
| Region XI | 2% (3) | 0 | 0 | 5% (7) | 0 | 0 | 5% (7) | 9% (14) |
| Total | 32% (50) | 1% (1) | 23% (35) | 18% (28) | 1% (1) | 2% (3) | 12% (18) | 100% (154) |
Table 3. Breakdown of respondents into regions and service capacity.
Source: Authors' compilation based on statistical results
Survey results
Our survey findings present important insight into the challenges and needs of the respondents. Participants from different parts of the country, ownership types, and service capacities offered a broad spectrum of issues in servicing vulnerable populations. Our findings validated major concerns that have been prevalent among HCFs for a long time.
Physical infrastructure. Almost all HCFs show compliance with physical infrastructure indicators. They conform to the accessibility specifications in their corridors, walkways, and doors. There are also adequate water closets or toilets for the public and staff. Most have provisions for breastfeeding areas, temperature scanning, hygiene, and disinfection supplies, including non-skid flooring. Additionally, the HCFs post directional signage that follows DOHs' Signage Systems Manual for Hospitals and Offices standards. However, Table 4 shows four indicators with significantly low compliance. These include diaper-changing areas and vending machines for hygiene commodities like sanitary napkins. Most HCFs comply with positional, directional, and warning tactile blocks for blind people. It was also seen that there is a lack of culturally sensitive areas for IP/ICC visitors and personnel.
Although the respondents generally comply with the DOH standards for health facilities, many expressed the need to upgrade their respective buildings. This is because most of the existing infrastructure was constructed without considering the needs of vulnerable groups, particularly PWDs. Only a few hospitals have dedicated rooms for IPs/ICCs and patients involved in GBV and VAWC cases. Additional fixtures, such as ramps, handrails, grab bars, and signages, must be installed, and appropriate space for corridors and bed capacity must be reviewed.
One of the major challenges among HCFs is their old structures. For example, one hospital is said to be seventy years old. Compliance with some standards and guidelines, especially recent issuances, is difficult due to this factor. There is an urgent need to develop a physical plan for repairs and renovations to incorporate requirements for accommodating vulnerable groups like PWDs. However, improving physical infrastructure would require mobilizing a great deal of resources. The availability of physical space is one aspect to consider in HCF plans for new offices, rooms, and areas dedicated to vulnerable populations. Nonetheless, many respondents noted that their facilities had limited space for upgrading. Some parts have also been converted into treatment and triage areas for COVID-19 patients. Therefore, hospitals face the challenge of modifying their infrastructure to create needed services and facilities for vulnerable groups, as indicated in the assessment tool. Those participants with ongoing renovations or construction plans admitted that some services and areas would be affected. The pandemic has delayed muchneeded repairs to attend to the needs of COVID-19 patients. The self-assessment taught them about requirements that cater to vulnerable groups, which the hospitals would consider during construction.
Table 4. Overall physical infrastructure compliance of HCFs (n = 154).
| Indicator | Complied (%) | Not complied (%) | |
|---|---|---|---|
| PI1 | Entry ramps | 80 | 16 |
| PI2 | Handrails | 77 | 20 |
| PI3 | Corridors | 89 | 8 |
| PI4 | Walkways | 90 | 7 |
| PI5 | Multi-level ramps | 68 | 23 |
| PI6 | Functional elevators | 44 | 32 |
| PI7 | Parking space | 72 | 24 |
| PI8 | Main door specifications | 95 | 5 |
| PI9 | Emergency exits | 93 | 7 |
| PI10 | Water closet standards | 76 | 20 |
| PI11 | Water closet fixtures | 56 | 40 |
| PI12 | Toilet-to-patient ratio | 85 | 12 |
| PI13 | Separate water closets for staff, patients, and visitors | 92 | 6 |
| PI14 | Separate water closets per gender | 77 | 20 |
| PI15 | Water closet/toilet per floor for PWDs | 75 | 19 |
| PI16 | Waste bins in water closets/toilets | 94 | 3 |
| PI17 | Diaper changing areas in water closets/toilets | 30 | 67 |
| PI18 | Facilities/vending machines with hygiene products | 27 | 71 |
| PI19 | Non-skid/slip floors | 91 | 7 |
| PI20 | Accessible seating for PWDs | 80 | 19 |
| PI21 | Tactile blocks for the blind | 23 | 75 |
| PI22 | Private room for GBV, VAWC, and HIV/AIDS cases | 64 | 33 |
| PI23 | Location/breastfeeding areas | 86 | 10 |
| PI24 | Culture-sensitive unit/area for IPs/ICCs | 18 | 74 |
| PI25 | Perimeter fence | 69 | 27 |
| PI26 | Hygiene materials | 98 | 1 |
| PI27 | Temperature-scanning device | 98 | 1 |
| PI28 | Directional signages | 93 | 5 |
| PI29 | DOH's Signage Systems Manual compliance | 88 | 11 |
| PI30 | Express lanes for vulnerable groups | 80 | 19 |
| PI31 | Waiting area | 79 | 19 |
Note: PI = physical infrastructure. (Source: Authors' compilation based on statistical results)
Another roadblock we cited under physical infrastructure involves process or procedural barriers. LGU-managed facilities have to undergo a tedious process, starting with a project proposal that will be reviewed for approval and fund availability. Similarly, the long procurement process contributes to delayed implementation. Private hospitals usually depend on the owner's support and discretion. In the case of some health centers, they raised concerns regarding temporary locations that require them to pay rent on top of direct costs.
Respondents unanimously point out financial limitations as the biggest constraint. Improvements in facilities or expansion of new spaces require investment. The COVID-19 emergency has also resulted in financial difficulties that forced HCFs to prioritize supplies and equipment for personnel protection, such as PPEs, purifiers, and temporary hospital wards. Additionally, respondents believe that facilities and services maintenance for vulnerable groups can be a cost
center. Despite financial constraints, participants would continue to include interventions for this sector in their annual investment plans and lobby their respective principals for consideration.
Equipment. We listed in Table 5 the respondents' overall compliance with the equipment component. There is high compliance among HCFs in five out of the seven indicators. However, there is a high percentage of non-compliance with the availability of culture-sensitive equipment accessible to IPs/ICCs. Moreover, there are slightly more non-compliant HCFs about having a database on telemedicine users.
| Indicator | Complied (%) | Not complied (%) | |
| E1 | Ambulatory care devices | 85 | 13 |
| E2 | Audio and visual alarm systems | 70 | 29 |
| E3 | Hotlines for COVID-19 and violence/harassment/abuse concerns | 79 | 21 |
| E4 | Device for telemedicine and virtual sign language interpretation | 68 | 32 |
| E5 | Stable signal and/or internet access | 69 | 30 |
Table 5. Overall equipment compliance of HCFs (n = 154).
Note: E = equipment. (Source: Authors' compilation based on statistical results)
E6 Database of telemedicine users 48 50 E7 Culture-sensitive equipment for IPs/ICCs 12 77
Aside from financial constraints, the HCFs attribute the absence of some of the listed equipment to their service capacity. This is one of the items of feedback we solicited from infirmaries and level-I hospitals participating in the assessment. They only offer basic services and facilities based on the category granted to them. Despite this, they assured their compliance with the minimum standards for the availability of ambulatory care devices for emergency cases, functional and dedicated hotlines for specific concerns, and telemedicine services. Additionally, some infirmaries agreed to apply to upgrade their category, which will lead to offering facilities and services to vulnerable groups.
From the survey, most of the equipment that HCFs would like to acquire include specializing in diagnostics, such as CT-scan, MRI, ultrasound, and COVID-19 testing. During the assessment, they were made aware of the units important to vulnerable groups, most often culture-sensitive equipment for the IPs/ICCs. Installation of PWD-friendly equipment, especially for the visuallyand hearing-impaired, is being considered, particularly telemedicine, braille systems, virtual sign language interpretation services, and visual and alarm systems.
On the other hand, a stable and fast internet connection should be present for some of the equipment to be operational. Most respondents complained of slow and intermittent connectivity. Sometimes, the facilities have 'dead spots' where the signal is unstable. This is why some HCFs are not fully equipped with telemedicine facilities.
As initially explained, one of the bottlenecks is the procurement process. Similar to acquiring equipment, the respondents cited delays relative to the administrative and logistic processes. Sometimes, the purchase would prioritize those units that are needed urgently. There are instances when the requested equipment or maintenance ancillaries are unavailable from the suppliers. Another concern mentioned is the need for an additional warehouse for storage. Lastly, the facilities' location and distance can affect the delivery delay.
Personnel capacity. Table 6 shows the comparison across personnel capacity's fifteen indicators. There are nine indicators that have more non-compliance, as indicated by the participants. The highest percentage of non-compliance is for the Filipino sign language interpretation training.
Meanwhile, from the six indicators with more compliance, the HCFs are highly compliant with knowledgeable and trained personnel in health promotions. We discuss the results for the personnel capacity indicators below.
Table 6. Overall personnel capacity compliance of HCFs (n = 154).
| Indicator | Complied | Not complied | |
|---|---|---|---|
| (%) | (%) | ||
| PC1 | Staff trained on telemedicine operation | 51 | 47 |
| PC2 | Staff trained on disability sensitivity and sign language interpretation | 27 | 71 |
| PC3 | Regular training on Filipino Sign Language (FSL) interpretation | 14 | 84 |
| PC4 | PWD referral pathway and helpdesk | 45 | 54 |
| PC5 | Staff trained on gender-responsive health service delivery | 51 | 49 |
| PC6 | Women and children protection unit (WCPU) with trained staff | 51 | 49 |
| PC7 | Referral pathway for GBV and VAWC cases | 58 | 42 |
| PC8 | Regular training on GAD, GBV, and VAWC | 38 | 62 |
| PC9 | Staff trained on providing services to IPs/ICCs | 24 | 75 |
| PC10 | Dedicated unit and referral pathway for IP/ICC-related concerns | 29 | 70 |
| PC11 | Regular training on culture-sensitivity | 16 | 82 |
| PC12 | Training on empathetic communication and RCCE | 23 | 77 |
| PC13 | Dedicated staff trained in health promotion | 67 | 32 |
| PC14 | Dedicated staff coordinating with the health promotion unit of the | 53 | 45 |
| local health office | |||
| PC15 | Dedicated mental and psychological support unit with trained staff | 49 | 51 |
Note: PC = personnel capacity. (Source: Authors' own compilation based on statistical results)
One of the important concerns from the assessment was the shortage of personnel in the HCFs. In addition to budgetary constraints, recruitment was difficult due to the pandemic. The respondents reported high demand for healthcare workers, such as doctors, nurses, and medical technicians, particularly during surges. Due to the limited personnel, hospitals could not assign dedicated staff to respond and provide services to patients from vulnerable groups. Their personnel had to prioritize urgent concerns regarding COVID-19, which usually fell on local health workers.
The pandemic also interrupted the personnel's capacity building. Sometimes, virtual training and seminars were limited or restricted because hospitals were busy with the patient influx. The respondents recognized the need to plan and conduct learning and development interventions to equip their personnel for programs and services that respond to recent developments and emerging concerns in the health sector.
All HCFs expressed willingness to attend available and free capacity-building activities, especially from DOH. They would like their personnel to take regular modules on cultural sensitivity regarding IPs/ICCs, handling GAD cases, GBV, VAWC, and other topics involving vulnerable groups. This also pertains to competencies related to PWD concerns, such as Filipino sign language and psychosocial support. Other areas of interest include health education, promotions, and IT/digital communications. For this purpose, the HCFs were requesting access and information on learning and development interventions from the DOH Academy.
Health promotions. The last component in the self-assessment was health promotion. This measured the compliance and availability of information materials, in various types and forms, that are necessary and accessible to vulnerable populations. There are nine indicators under this component. Table 7 shows that most indicators are complied with by the participants. Two
indicators have low compliance: the availability of information materials on gender-related concerns services, GBV, VAWC, and translated materials for dominant IPs/ICCs in the area.
| Table 7. Overall health promotion | compliance of HCFs (n | = 154). |
|---|
| Indicator | Complied (%) | Not complied (%) | |
|---|---|---|---|
| HP1 | Visual promotion materials on COVID-19 | 94 | 6 |
| HP2 | Recorded audio promotion materials on COVID-19 | 64 | 36 |
| HP3 | Printed visual instructional materials on COVID-19 testing | 85 | 14 |
| HP4 | Visual materials on hand hygiene and sanitation | 97 | 3 |
| HP5 | Recorded audio materials on COVID-19 prevention measures | 62 | 38 |
| HP6 | Printed materials on PWD series | 54 | 46 |
| HP7 | Printed materials on services for gender-related concerns | 46 | 54 |
| HP8 | Printed materials on sexual and reproductive health services | 68 | 32 |
| HP9 | Printed translated materials for IPs/ICCs | 27 | 72 |
Note: HP = health promotion. (Source: Authors' own compilation based on statistical results)
We found that respondents rely on the DOH for official promotional materials. However, the limited platform and delivery delays have caused them to seek alternative sources. Additionally, the lack of IEC materials for vulnerable groups is a concern. The pandemic has deprioritized the production of health promotion materials, resulting in a shift toward social media dissemination. However, connectivity issues also pose a challenge. HCFs suggest implementing policies prioritizing health promotion. Continuous training can augment IEC materials, and PCERP's selfassessment survey is relevant to monitor adaptability. Despite resource mobilization challenges, HCFs prioritize public service, especially for vulnerable groups.
Inclusivity checklist for health promotion playbooks. Concerning the requirements for health promotion, part of the self-assessment tool was the HCFs' engagement with its respective stakeholders, especially with the vulnerable sector, for its information and education programs. The additional section was based on the inclusivity checklist for health promotion playbooks developed by DOH's Health Promotion Bureau. We present the major results from this component in Table 8. Most healthcare facilities responded positively to involving vulnerable groups in the planning process. Some HCFs mentioned initiating hospital-based health promotion playbook programs, organizing key committees, and conducting surveys or feedback activities. Despite pandemic challenges, HCFs expressed their intention to resume consultations with vulnerable groups for ongoing and future programs.
Table 8. Overall health promotion playbook compliance of HCFs (n = 154).
| Response | % | |
|---|---|---|
| Complied | 76 | |
| Not complied | 14 | |
| Not applicable | 10 |
Note: HPP = health promotion playbook. (Source: Authors' own compilation based on statistical results)
The respondents largely viewed their interventions as non-discriminatory, with a comment emphasizing the need for more emphasis on sexual orientation and gender identity guidelines. Compliance with non-discriminatory practices was high overall. The table also indicates significant compliance with the strategic placement of information, education, and communication materials within facilities. Some HCFs mentioned limited availability of IEC materials but implemented solutions like additional bulletin boards and multimedia platforms.
Most agreed on the need for dedicated space for sensitive cases, while some mentioned regular reviews of safety protocols. Responses varied for this requirement. Most participants also expressed non-compliance regarding the availability of communication materials for vulnerable groups. Limited types of accessible IEC materials were reported, prompting plans for capacity building in sign language interpretation and including vulnerable groups' input through surveys.
Respondents had translated training modules and communication materials for their communities, but a significant percentage were non-compliant or found the question non-applicable. Reasons included materials being available only in selected translations. The results also showed that most HCFs provided good placement of information and education materials without physical barriers, unaffected by health and safety protocols. The majority also expressed compliance with the absence of procedural barriers. However, some mentioned potential red tape from other agencies and the lack of necessary machines and equipment for patient care.
Discussion
Our results align with previous literature emphasizing the need for multifaceted approaches to improve healthcare accessibility for vulnerable groups. The self-assessment we used identified gaps across physical infrastructure, equipment, personnel capacity, and health promotions similar to management deficiencies found in studies by Thangaraj and Loganathan (2021), Ahmad et al. (2021), Gudlavalleti (2019), Velasco et al. (2021), and Marella et al. (2016). We bring to the fore the value of assessment tools like the self-assessment survey we used here for evaluating facilities' capacity to serve vulnerable populations (Carter et al., 2021). Targeted improvements can be targeted by identifying specific gaps.
We found that our results relate to factors in the Andersen behavioral model that influence healthcare utilization. Deficiencies in physical infrastructure and equipment correspond to a lack of enabling resources, while gaps in personnel capacity reflect insufficient predisposing factors. We present the direction for interventions to improve enabling factors and address predisposing barriers by integrating our results with the ABM. Our results, however, diverged from the literature regarding the role of community health workers, which has been emphasized as an impactful intervention (Carter et al., 2021; Kuper et al., 2021; Bhatt & Bathija, 2018). We found that few facilities reported establishing partnerships with community health workers.
Although the literature highlighted stigma and transportation as significant barriers to healthcare access, we did not directly evaluate these factors in our self-assessment. We acknowledge this as a limitation, as the ABM indicates that predisposing and enabling factors contribute to utilization. Our results confirm and expand upon known challenges in healthcare accessibility for vulnerable groups. We present theoretical grounding to shape supportive policies, programs, and interventions based on the ABM lens. Additionally, the small sample size of HCFs participating in the self-assessment survey limited the generalizability of the findings to other HCFs in the country. Additionally, we did not examine the impact of the HCF self-assessment on the quality of healthcare services provided to vulnerable groups, which is a limitation of concern in our study.
Despite these limitations, our findings have significant policy implications for enhancing access to healthcare services for vulnerable groups in the Philippines. The identified gaps and deficiencies in healthcare facilities' capacity to serve vulnerable populations underscore the need for targeted interventions and policies. For instance, policies mandating the installation of ramps, handrails, and accessible toilets in healthcare facilities can address the lack of physical infrastructure accommodations for PWDs. Similarly, policies prioritizing the procurement of assistive equipment and technology can improve accessibility for vulnerable groups. Moreover, regular training for healthcare personnel on cultural sensitivity, disability awareness, and genderresponsive care should be required to enhance their capacity to serve diverse populations. Previous studies have demonstrated the effectiveness of similar interventions and policies in improving healthcare accessibility for vulnerable groups. For example, Ganle et al. (2020) found that training healthcare providers on disability-inclusive care improved access to services for PWDs in Ghana. Similarly, Marasinghe et al. (2015) reported that policies promoting the availability of assistive devices enhanced healthcare accessibility for older adults.
Conclusion
The COVID-19 pandemic has exposed and exacerbated existing inequalities in healthcare access, underscoring the urgent need to address the accessibility of healthcare services for vulnerable groups in the Philippines. Our study's findings exhibit significant gaps and deficiencies in healthcare facilities' capacity to serve these populations, highlighting the importance of investing in targeted interventions and policies. Enhancing healthcare accessibility for vulnerable groups is not only a moral imperative but also crucial for promoting health equity and building resilience in the face of future health emergencies. Moreover, it aligns with the Philippine government's commitment to achieving universal health coverage and the Sustainable Development Goals.
Our study has important theoretical and practical implications. Theoretically, our research contributes to the understanding of healthcare accessibility by applying the Andersen behavioral model to examine the predisposing, enabling, and need factors influencing healthcare utilization among vulnerable groups. ABM is our lens for understanding the complex interplay of factors affecting access to healthcare services and highlights the importance of addressing these factors to improve accessibility for vulnerable populations. Practically, our findings suggest a need to increase participation in the HCF self-assessment survey to obtain a more comprehensive understanding of the situation in the country.
We recommend modifying the self-assessment tool based on the service capacity of HCFs to monitor compliance with standards more accurately and identify deficiencies in each category. Additionally, we emphasize the importance of patient/client feedback in improving HCF services and the need for a comprehensive action plan to support the HCF self-assessment initiative. We also recommend conducting regular sectoral meetings as an approach to stakeholder engagement to obtain relevant information on the ground, which can be used as input for policy-making and strategic plans concerning vulnerable groups.
In light of our findings and the compelling evidence from other studies, we call upon policymakers, healthcare administrators, and stakeholders to prioritize the development and implementation of policies and interventions that enhance healthcare accessibility for vulnerable groups in the Philippines. By doing so, we can ensure that no one is left behind in the pursuit of health and well-being and build a more equitable and resilient healthcare system for all. Future research could explore the effectiveness of the HCF self-assessment initiative in improving the accessibility of healthcare services for vulnerable groups, investigate the factors contributing to the low participation rate in the self-assessment survey, and examine the impact of patient/client feedback on the quality of healthcare services provided by HCFs.
Abbreviations/acronyms
ABM: Andersen behavioral model; COVID-19: infectious disease caused by the SARS-CoV-2 virus; DILG: Department of Interior and Local Government; DOH: Department of Health; DOH-FAQs: frequently asked questions; GAD: gender and development; GBV: gender-based violence;
HFCs: healthcare facilities; HIV/AIDS: human immunodeficiency virus/acquired immunodeficiency syndrome; ICCs: indigenous cultural communities; IEC: information, education, and communication; IPs: indigenous peoples; LGBTQIA+: lesbian, gay, bisexual, transgender, queer, intersex, asexual; NCIP: National Commission on Indigenous Peoples; NCR: National Capital Region; PA: public address; PCERP: Philippines COVID-19 Emergency Response Project; PWDs: persons with disabilities; RCCE: risk communication and community engagement; UNICEF: United Nations Children's Fund; VAWC: violence against women and their children; WCPU: women and children protection unit; WHO: World Health Organization.
Acknowledgment
We want to express our sincere gratitude to our respective institutions for their invaluable support in our research on improving the accessibility of healthcare facility services for vulnerable populations.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Declarations
The authors declare that the research was conducted without any commercial or financial relationships that could be construed as a potential conflict of interest.